The end product of all the hard work of the hair follicle is the “hair strand” which we all are familiar with. Humans have about 90,000 - 100,000 of these on the scalp. Individuals with hair loss have less.
All of the machinery to make a hair lies below the scalp surface. Hairs typically extend 4-7 mm below the surface. It varies from patient to patient - and even varies to some degree for the same patient. The longest hairs on the scalp are the so called terminal hairs. The lie deep down in the fat layer.
During the process of balding, hairs not only becomes skinnier and skinnier (miniaturized) but they becomes shorter and shorter. The so callee vellus-like hairs of androgenetic alopecia no longer live deep down in the fat layer. Rather these hairs are found higher up in the dermis. These vellus hairs may only be 2 mm long and 10 mm thick in some cases compared to 6-7 mm long and 80 micrometer thick terminal hairs.
This article was written by Dr. Jeff Donovan, a Canadian and US board certified dermatologist specializing exclusively in hair loss.
The scarring alopecias are a group of hair conditions associated with the development of scarring under the scalp. Hair loss is often permanent although treatment might help slow or stop the loss.
A variety of means are available to reduce the appearance of hair loss for patients with scarring alopecia. These include wigs, hairpieces, hair systems, hair fibers, DermMatch, scalp micopigmentation and of course the method of hairstyle.
Trichoscopic image of DermMatch concealer on the scalp in a patient with folliculitis decalvans (a scarring alopecia)
All methods have their unique advantages and disadvantages. Patients with scarring alopecias who are applying medications daily may find thicker powdercakes like “DermMatch” less convenient than hair fibers because they are just a bit more difficult to wash off and most certainly do block topical medications from properly reaching the scalp. Patients with scarring alopecia have inflammation in the scalp and factors such as irritation from fibers, itching/irritation from the use of wigs during hot days and fading of scalp micopigmentation pigments must all be taken into consideration when choosing a camouflage method.
This article was written by Dr. Jeff Donovan, a Canadian and US board certified dermatologist specializing exclusively in hair loss.
Active vs Inactive Scarring Alopecia: Which do I have?
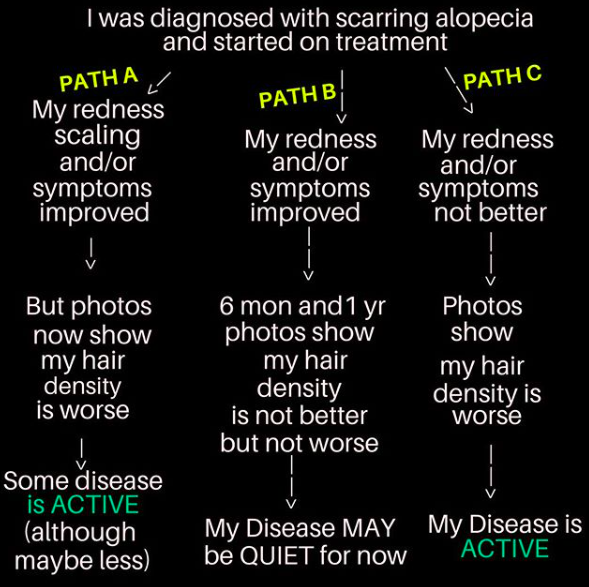
There is often a lot of confusion about whether or not a person’s scarring alopecia is active or not. A good rule is this: If a photograph of the scalp taken 2 years apart shown absolutely no change in density - the scarring alopecia is probably quiet. Now that could be quiet because the medications made it quiet or quiet because it truly is in remission or “burnt out.” If a photo taken 6 months from the last shows that there has been more hair loss, the scarring alopecia is probably still active. Of course one needs to consider the possibility that another hair loss condition like a telogen effluvium or worsening androgenetic alopecia is the reason the hair is worse. But in general, if the hair is worse, there is a good chance it’s due to the scarring alopecia being active. Patients often comment that their redness is better or their symptoms are better after treatments. That’s wonderful news of course but what really matters is whether the hair is still disappearing from the scalp week by week and month by month.
SCARRING ALOPECIA FLOW CHART
The above diagram is a helpful diagram. In “Path A” the patient feels better about the way their scalp looks or feels but they still appear to be losing hair. It’s important not to get overconfident that treatment is a major success. It might be helping (ie partial treatment success) but things are still active. In “Path C” it’s clear things aren’t working. The patient is worse and unless treatment is changed we’re in for more hair loss. In “pathway B” we seem to have halted the disease. After 6 months, it’s hard to say with 100 % confidence that we’ve stopped the disease (as maybe it’s just slowed it down but not halted). If there is absolutely no change in the hair density after 1 full year, there’s a pretty good chance we can celebrate a bit. Of course it would be nice if we could get an improved density but that is not always the goal in scarring alopecia. Even after one year, we need to keep in mind that maybe the disease is a tiny bit active and the camera can’t pick up these differences. After two years however, if the before and after photos 24 months apart look 100 % identical - the disease is highly likely to be quiet or “inactive.”
This article was written by Dr. Jeff Donovan, a Canadian and US board certified dermatologist specializing exclusively in hair loss.
Lichen planopilaris (LPP) is a type of scarring alopecia. It affects both men and women and typically those 30-60 years of age. The diagnosis becomes easier over time for any given patient given that time may allow certain characteristics to develop around hairs (ie perifollicular scale or perifollicular redness) and time may also allow areas of hair loss to develop on the scalp.
The earliest stages of LPP are more challenging to correctly identify. The early diagnosis is, however, quite important to reduce the progression of the hair loss. In addition, this is the stage at which some amount of improvement might still be possible with aggressive treatment. A few key concepts will allow the astute physician to pick up on clues that will them prompt a scalp biopsy (which can then potentially help rule in or rule out the diagnosis). These clues include (1) reports by the patient of itching of the scalp along with burning or tenderness (2) redness in the scalp along with excessive shedding. For many patients, LPP declares its presence with unpleasant symptoms along with increased shedding of hair. It can mimic seborrheic dermatitis almost perfectly as it did in this patient shown here.
This article was written by Dr. Jeff Donovan, a Canadian and US board certified dermatologist specializing exclusively in hair loss.
“Do you think I have frontal fibrosing alopecia (FFA)?” 10 years ago it would be rare for a patient to spontaneously ask this question. Now it’s common. Paralleling the rise in the number of cases worldwide of FFA being diagnosed is the increase in awareness of this condition. FFA is still rather rare with anywhere from 1:5000 to 1:10000 people affected (my estimate) depending on the country.
Diagnosis of FFA is more than simply “I think my hairline is changing.” After all, the “I think my hairline is changing” patient could have androgenetic alopecia, traction alopecia, alopecia areata, trichotillomania, lupus, or telogen effluvium ... or 20 other conditions too.
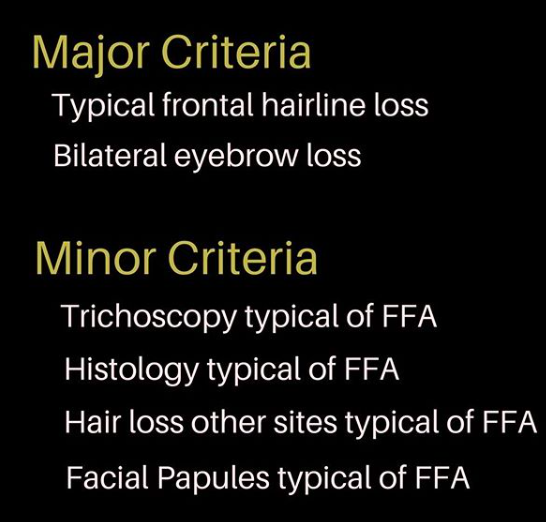
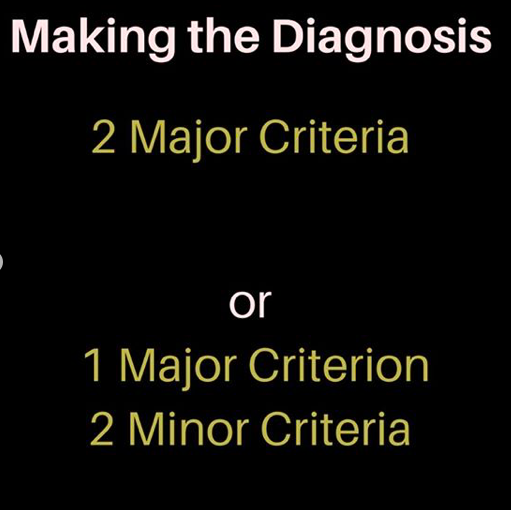
Criteria for FFA have been suggested in recent times. The 2 major criteria focus on the classic hairline changes and classic eyebrow changes. The minor ones pertain to trichoscopy, histology and two other clincial features - the loss on other areas of body and the so called facial papules. Diagnosis requires 2 major criteria or 1 major and 2 minor.
Does this patient have FFA or not?
The patient in this photo above does not have FFA. She has frontal hairline loss but it is not scarring. She has miniatured and vellus (small pale hairs) that are typical of androgenetic alopecia but would be unusual for FFA. She has eyebrow loss from over shaping and tweezing but not from FFA. Her dermoscopy does not favor FFA and she does not have hair loss on other sites that is in keeping with FFA not does she have facial papules.
This article was written by Dr. Jeff Donovan, a Canadian and US board certified dermatologist specializing exclusively in hair loss.
We are just beginning to understand the role of inflammatory factors in male balding (androgenetic alopecia). Although the story of male balding has focused on the role of dihydrotestosterone (DHT) for almost 40 years, new avenues are being explored / especially those pertaining to inflammation.
It’s clear that reducing inflammation helps male balding. (Drug companies like Aclaris hope it helps a lot as they go about studying JAK inhibitors to fight inflammation in male balding). The problem is still that we don’t fully understand how best to reduce inflammation. Eating an aspirin with dinner as a means to block inflammation won’t help. However, new data suggests filling the dinner plate with a giant salad rich in raw vegetables and herbs just might.
New Study Suggests Raw Vegetables and Herbs May Have a Role to Slow Balding
A 2018 study from Italy examined factors that could be relevant to balding in males. Researchers performed a case control study of 104 males with balding and 108 controls without balding. The study revealed that diets rich in raw vegetables and fresh herbs reduced the risk of balding. The authors of the study suggested that eating raw vegetables and herbs could potentially have a role to reduce the onset and progression of male balding.
I really enjoyed discovering and reading this study. All dietary studies have their flaws (and in fact all studies). Critics will love to pounce on this one (and in fact pounce on all studies). But this is a study which sets the stage for some further carefully designed studies moving forward. If a drug was available that could safely reduce the onset and progression of male balding to the degree shown in this study, it would be a big seller. It would receive approval in no time and would be a household name. The good news is that the supermarket rather than the pharmacy may in fact be the place to find such products already. More studies are needed.
Reference
Fortes et al. Mediterranean diet: fresh herbs and vegetables decrease the risk of Androgenetic alopecia in males. Arch Dermatol Research 2018; 310;71-76
This article was written by Dr. Jeff Donovan, a Canadian and US board certified dermatologist specializing exclusively in hair loss.
Diet and Seborrheic Dermatitis: New Pieces of the Puzzle
Depending on how slow (or fast) one eats and how much (or little) one eats, most people spend about 4 % of their lives consuming food. It should come as no surprise that diet can influence many health issues - including various hair conditions. However, the extent to which diet really impacts hair & scalp disorders is only just starting to be properly examined by researchers.
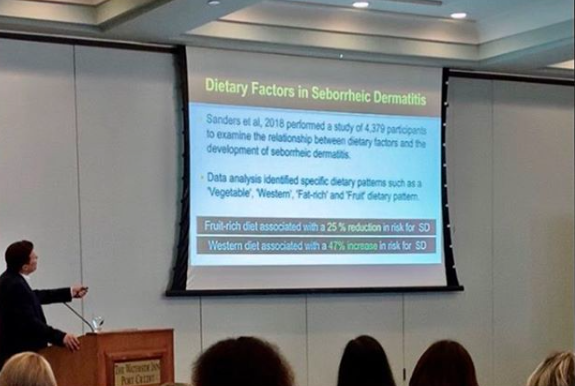
Dr. Donovan lecturing at the 2019 World Trichology Conference
At the 2019 World Trichology Conference (pictured above), I had the opportunity to speak to conference delegates about a few of these issues. Here, I am speaking to the audience about a fascinating study from Sweden which provided some nice evidence that diet really can impact the scalp. This study showed that a diet rich in fruit was associated with a 25 % reduction in the risk for seborrheic dermatitis and a more typical “Western” diet (which the authors classified as a diet high in meat, potatoes, alcohol) was associated with an increased risk for seborrheic dermatitis - particularly for females. It is proposed that the inflammatory potential of our foods may influences these trends. Other factors may also be involved. Studies of dietary factors are challenging to conduct but have profound impact on multiple aspects of human health.
Reference
Sanders et al. Association Between Diet and Seborrheic Dermatitis: A Cross Sectional Study. Journal Investigative Dermatology 2019; 139: 108-114
This article was written by Dr. Jeff Donovan, a Canadian and US board certified dermatologist specializing exclusively in hair loss.
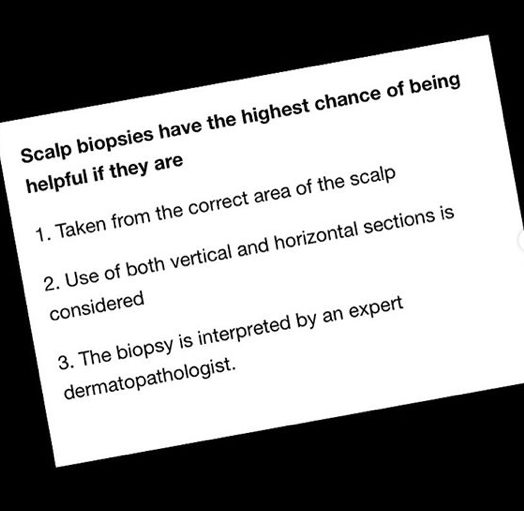
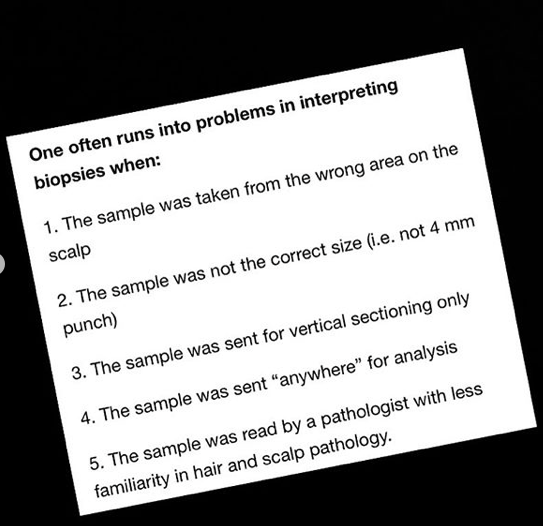
Scalp biopsies can be very helpful tools when they are used in a correct manner. If a biopsy is going to be done, the correct spot on the scalp needs to be chosen, using the correct biopsy technique and sent to the correct lab for the correct type of processing so that interpretation can be done by the correct pathologist.
As I have discussed several times before, there are several factors which enhance the accuracy of a biopsy
Hair Casts in Inflammatory Scalp Disease: A Closer Look at Seborrheic Dermatitis
“Hair Casts” are thin elongated tubular like structures that wrap around the hair shaft. They are generally 2-7 mm in size.
Appearance of hair casts by trichoscopy in a patient with seborrheic dermatitis
Hair casts are said to be “primary” when not associated with any underlying scalp condition and “secondary” when associated with an underlying scalp issue. A variety of inflammatory and non inflammatory conditions lead to hair casts including seborrheic dermatitis(shown here), psoriasis, traction alopecia, scarring alopecia, pemphigus, hair sprays and more. Treatment is centred around treating the acual underlying disorder. For this patient treatment of the seborrheic dermatitis with a combination of zinc pyrithione and ciclopirox shampoos together with a topical steroid containing salicylic acid helped lead to resolution.
This article was written by Dr. Jeff Donovan, a Canadian and US board certified dermatologist specializing exclusively in hair loss.
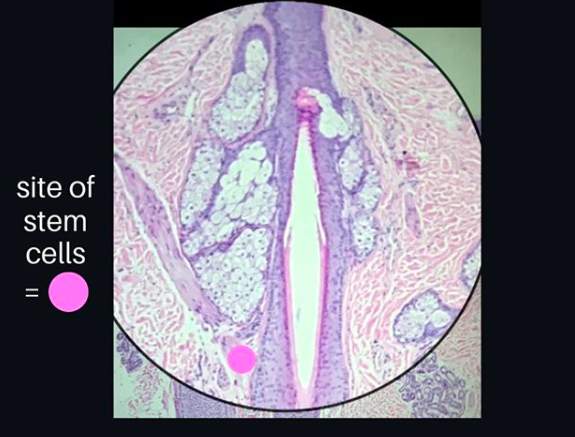
Hair follicle stem cells are cells with the potential to generate new hairs and potentially even other tissue types as well. There is an incredibly important area of the hair follicle where stem cells live. This area is known as the “bulge” and is located where the arrector pili muscle inserts into the outer root sheath (see pink dot in diagram). It was Dr George Cotsarelis, together with Dr Robert Lavker who discovered back in 1990 that the bulge was the location where hair follicle stem cells reside. Dr Cotsarelis was a dermatology resident at the time he made these breakthrough discoveries. He has since contributed to some of the most important discoveries in hair research in recent times.
Reference
Cotsarelis G et al. Label-retaining cells reside in the bulge area of pilosebaceous unit: implications for follicular stem cells, hair cycle, and skin carcinogenesis. Cell. 1990.
This article was written by Dr. Jeff Donovan, a Canadian and US board certified dermatologist specializing exclusively in hair loss.
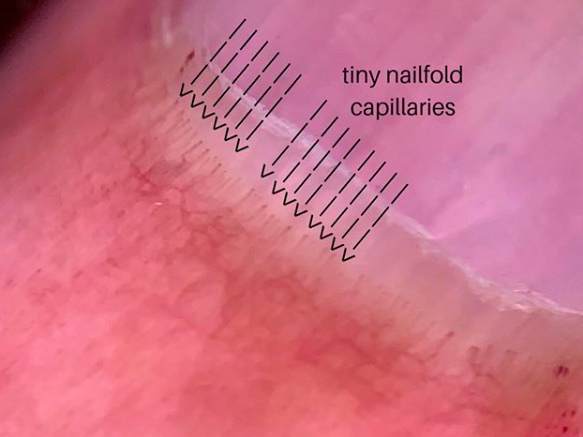
For the hair dermatologist, the nails are important to examine when examining the patient. The shape and appearance of the nails are important and so are the nail folds -(the area where the nail first starts as one moves down from the knuckles towards the end of the finger). It is the appearance of the tiny blood vessels in the nail folds that are so important to examine in patients with suspected autoimmune disease.
Examination is done with a dermatoscope and the practice of doing this is simply referred to as “nail fold capillaroscopy.”
Normal Nailfold Capillary Arrangement (by dermoscopy)
This photo above shows the normal arrangement of these nail fold capillaries. They are all the same thickness and straight and lined up in a regular manner. Extremely important is the fact that none are missing. Dilation of these tiny capillaries and “dropout” whereby many start disappearing can be a sign of more serious underlying disease. Changes in the capillaries have been studied in detail in autoimmune diseases like dermatomyositis, psoriasis, lupus and scleroderma - and the precise appearance may help predict underlying organ disease. For example, in children with the skin disease dermatomyositis, reduced nailfold capillary density was associated with the children and teens having lung disease. In scleroderma, there is an association with lower capillary density and death. Other examples continue to be discovered.
This article was written by Dr. Jeff Donovan, a Canadian and US board certified dermatologist specializing exclusively in hair loss.
Scalp Trichoscopy: Essential to the Practice of Hair Dermatology
Few people would argue that good binoculars aren’t an essential part of being a bird watching enthusiast. I’m not a birder myself but you can spot a bird watcher quite easily. The binoculars, the cameras, the gear. It all goes together. Even the shoes. There are essential tools to this particular hobby.
I don’t use binoculars in the clinic to examine hair. But I do use a set of lenses and an instrument known as a “dermatoscope.” A dermatoscope is more than just a magnifying glass - it uses magnifying optics along with various types of lighting sources. Surprisingly, it is still a bit of a debate for some practitioners as to whether one really needs a dermatoscope to practice in the field of “hair dermatology”. The purpose here is not to force the idea but rather to allow those who wish to think about the subject carefully to come to their own conclusions. I do not need binoculars to tell the difference between a bird or a squirrel that sits in the tree. But I do require binoculars to differentiate between all the subtle intricacies of birds that bird watchers so enjoy. Similarly, I do not need a dermatoscope to diagnose the cause of hair loss of most patients who walk through the door of my office. I do, however, require the dermatoscope to sort out the more challenging cases and to predict how even straight forward cases are likely to respond to treatment.
For my practice, a dermatoscope is essential.
This article was written by Dr. Jeff Donovan, a Canadian and US board certified dermatologist specializing exclusively in hair loss.
Diagnosing hair loss is like detective work. A detective solves mysteries by putting all the pieces of the puzzle together. The same is true for hair loss. A hair specialists comes to understand what diseases fit with certain descriptions and what diseases just don’t. What are the top 20 causes of a red scalp? What if we limit this question to asking about the top causes of a red scalp that bleeds? ... or a red scalp associated with rashes elsewhere on the body? or a red scalp associated with increased daily hair shedding? A specialist must always be able to scribble down a list of suspects and then figure out the actual cause.
This photo below shows a red scalp that is flaky and mildly itchy. It bleeds from time to time. Scalp psoriasis is a top cause but issues like seborrheic dermatitis, contact dermatitis, scarring alopecias and skin cancers must be kept in mind. If a certain disease is suspected but fails to actual respond to the treatment as one hoped it would ... a scalp biopsy should be taken.
This article was written by Dr. Jeff Donovan, a Canadian and US board certified dermatologist specializing exclusively in hair loss.
Perifollicular Scaling in Lichen Planopilaris (LPP)
Lichen planopilaris (LPP) is a scarring alopecia. Affected patients frequently develop hair shedding in the initial stages and this is often accompanied by itching, burning and/or tenderness in the scalp.
Areas of permanent scarring hair loss can be visualized on the scalp as the disease progresses. However, in the early stages, findings such as scalp redness, or redness around hair follicles (perifollicular erythema) or scaling around hair follicles (perifollicular scaling) may be the only signs of the disease. This patient has LPP and the scaling was initially mistaken for dandruff. The intense itching, burning and tenderness she was experiencing were among the clues that another condition besides dandruff might be present.
Trichoscopic image of lichen planopilaris showing typical scale around hairs (ie. perifollicular scale)
A biopsy is not always needed to diagnose LPP. If all the pieces of the puzzle fit, and the clinician is confident the diagnosis is indeed LPP, a biopsy does not add anything further and may not be necessary. However, if there is any uncertainty with the diagnosis or something just does not seem clear, a 4 mm punch biopsy should be performed to evaluate further.
This article was written by Dr. Jeff Donovan, a Canadian and US board certified dermatologist specializing exclusively in hair loss.
Every hair specialist who first learns how to diagnose hair loss first learns about something known as the “classical presentation.” This refers to the way the specific condition might be described in textbooks. Not surprising, the classic presentation is also referred to as the “textbook presentation” of the condition.
Physicians often say statements like “it was a classic presentation” or “the hair loss was textbook” reflecting the common use of these terms.
Despite this, we must remember that sometimes the way hair loss develops on the scalp hair is not quite classic. Sometimes, the patient in the next room does not have a textbook presentation. Alopecia areata, some scarring alopecias and even some types of hair loss from drugs show up on the scalp in ways we just don’t see as we flip through the textbooks. These are in essence variations on the classic or textbook presentation.
There is always some aspect of the disease that is still seen in these “non classic” presentations. Consider as an example the patient with the scarring alopecia lichen planopilaris who has little in the way of scalp scaling or redness yet shows clear pockets of evolving scarring. Or the patient without great amounts of miniaturization who is clearly thinning in a localized patterned distribution.
These sets of photographs of Canadian geese reminded me that we can generally figure out what’s going on if we consider everything in context - even if the presentation isn’t quite classic.
This article was written by Dr. Jeff Donovan, a Canadian and US board certified dermatologist specializing exclusively in hair loss.
One of the challenges in FFA has been developing a consistent method to monitor the condition. How to we measure changes in the hairline? What changes should be followed? How do we photograph? It’s clear that many dermatologists that specialist in hair loss have slightly different methods of monitoring the condition. Scales used for monitoring other scarring alopecia just don’t work in FFA.
The Frontal Fibrosing Alopecia Severity Index (FFASI)
In 2016, Holmes and colleagues published a scale known as the “Frontal fibrosing alopecia severity index (FFASI)” for monitoring changes in FFA. It evaluates FFA based on a score of 100. Points are assigned according to different level of hair loss along the frontal hairline. Additional points are given for patients with eyebrow, eyelash and various areas of body hair loss. The presence of lichen planopilaris on the scalp, facial papules and lichen planus on other areas of the body also give additional points.
Reference Holmes S, et al. Br J Dermatol. 2016
This article was written by Dr. Jeff Donovan, a Canadian and US board certified dermatologist specializing exclusively in hair loss.
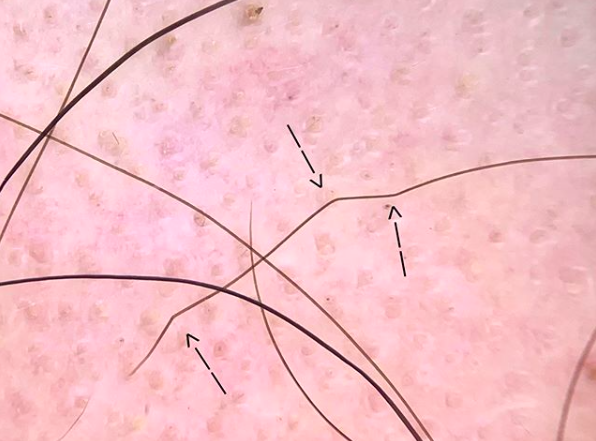
Alopecia areata is an autoimmune condition that affects about 2 % of the world in their lifetime. The condition is associated with inflammation that accumulates at the bottom of hairs deep under the scalp. This inflammation makes it difficult for hair to grow properly. Some hairs don’t grow on account of the inflammation and just fall out of the scalp. Some hairs grow for a bit but then simply snap off producing black dots. Other hairs are able to grow despite that fact that the manufactured hair fiber is so weak. Such fibers often show kinks and bends and may be referred to as “elbow hairs.” These hairs (see arrow in photo below) are quite weak and at increased risk for snapping off.
This article was written by Dr. Jeff Donovan, a Canadian and US board certified dermatologist specializing exclusively in hair loss.
Dupilumab is a treatment that helps patients with eczema (atopic dermatitis). Dupilumab is an interleukin 4 (IL-4) receptor α-antagonist that inhibits IL-4 and IL-13 signaling through blockade of the shared IL-4α subunit. The drug was approved by the US Food and Drug Administration in March 2017 and Health Canada in Dec 2017 for the treatment of adult patients with moderate to severe atopic dermatitis not adequately controlled with topical therapies. The drug blocks a group of white blood cells know as TH2 cells which are known to play a role in eczema.
Dupilumab has been reported to trigger hair regrowth in some patients with alopecia areata and atopic dermatitis (ie eczema).
In 2018, Penzi and colleagues reported that dupilumab helped regrow hair in a patient with alopecia totalis who was receiving dupilumab as treatment for their eczema. Several other case reports have now reported improvements in hair regrowth with dupilumab including reports by Smogorzewski and colleagues and Uchida and colleagues. Interestingly, some studies have reported development of alopecia areata during the course of treatment with dupilumab.
Side effects of dupilumab include injection-site reactions, conjunctivitis, blepharitis, oral herpes, keratitis, eye pruritus, other herpes simplex virus infection, and dry eye. The side effect of hair regrowth in patients with alopecia areata is serendipitous and likely will fuel further research in the use of this drug in alopecia areata.
Reference
Penzi et al.Hair Regrowth in a Patient With Long-standing Alopecia Totalis and Atopic Dermatitis Treated With Dupilumab. JAMA Dermatol 2018
This article was written by Dr. Jeff Donovan, a Canadian and US board certified dermatologist specializing exclusively in hair loss.
White Hairs in Regrowing Areas of Alopecia Areata: Why do they Occur?
Alopecia areata is an autoimmune disease that causes hair loss. The precise cause is not clear although it is clear that the immune system is activated to attack the hair. The target inside the hair follicle that the immune system is “going after” is still being debated by researchers. It may be one target or may be several. Among the theories is that proteins involved in the pigmentation of hair follicles are involved. We call the process melanogensis and researchers are focused on whether melanogenesis‐related peptides are among the autoantigens in alopecia areata.
White hairs are frequently see in regrowing areas in alopecia areatea
Alopecia areata may preferentially target ‘pigmented’ hairs
Clinically, we have come to understand that alopecia may preferentially affect pigmented hair and sometimes will leave any white hairs on the scalp unaffected. In extreme cases, a patient with a mixture of grey and colored hair will find that they go from having dark hair to stark white hair “overnight.” This is form of alopecia areata where the dark pigmented hairs fall out due to their attack by the immune system and the white hairs are unaffected.
White hairs may also be seen as hairs are trying to regrow in patients with alopecia areata. Small white hairs are commonly seen and this provides a nice example that the delicate hair has not yet figured out how to add color back into the hair. In other cases, the normal growing hair will lose it’s pigmentation at the bottom and start emerging from the scalp as a white color. That is shown here.
This article was written by Dr. Jeff Donovan, a Canadian and US board certified dermatologist specializing exclusively in hair loss.