Bad relaxer
I posted an answer to a new question on Realself.com
This article was written by Dr. Jeff Donovan, a Canadian and US board certified dermatologist specializing exclusively in hair loss.
Share This
I posted an answer to a new question on Realself.com
I posted an answer to a new question on Realself.com
Male pattern hair loss vs stress or nutrient related: how to tell?
I posted an answer to a new question on Realself.com
I posted an answer to a new question on Realself.com
I posted an answer to a new question on Realself.com
I posted an answer to a new question on Realself.com
I posted an answer to a new question on Realself.com
Over the years, I have made a few general assumptions in my clinic. I generally assume, for example, that the changes in appearance or emotion that accompany a person's hair loss really matters to any given patient who make an appointment with me. After all, why else would someone make the effort to book an appointment ?
Of course, any assumption will have it's exceptions and times where the assumption is not valid. Like the man who comes in because his wife or girlfriend asks him too make an appointment even though he is not really too bothered by his hair loss. Or the child who feels things are just fine but whose parent thinks there is something extremely wrong. Exceptions exist to any assumption and one must always be careful when making any type of assumptions.But generally speaking, most people who visit a hair physician value their hair.
"It's my crowning glory, Dr. Donovan"
"It's my best feature"
"I know you might not know by looking at me but I used to have five times the amount of hair I have now"
"I used to get so many compliments about my hair"
The list could go on and on.
And so it's fairly safe to assume that hair matters to the people who come see me. (In fact, it's a pretty safe assumption that hair matters to most humans at least for some duration of time even if just a passing thought).
The one assumption that is often incorrectly made by clinicians is that patients with more severe hair loss are more affected by the emotional impact of their hair loss. It sure sounds like a good assumption... except it's just not true. Some people with a small degree of hair loss can be similarly affected and sometimes even more emotionally affected than those with more significant amounts of hair loss. Study after study has shown that physicians wrongly assume they understand the impact of a patient's hair loss. Certainly assumptions can be wrong.
One of the reasons the assumption that "more hair loss means more impact" does not hold true is that we don't know everything about every patient. We strive of course to understand many things about the patient's medical history and all relevant related details. In fact, in my clinic I've been using a standard medical questionnaire for the past 7 years to gather all the relevant medical information from the patient. Despite this detailed medical questionnaire, we don't understand the complete picture of the patient. The questionnaire is only a fairly complete medical picture but lacks an ability to gather information about the psychosocial factors have influenced the patient in the past and are currently influencing his or her day to day.
Why does hair actually matter to the patient? What societal pressures (if any) does the patient feel? Does youthfulness, aging, and health in general carry with it emotional significance that is hard to describe or put to paper? Why does the patient sitting in front of me motivated to do something about the changed they see in their hair?
We as physicians don't always come to know all the details of everyone's story. Some stories and the details they contain are private and don't directly impact the diagnosis and treatment - and so they remain with the patient. Some issues aren't even fully understood by the patient ... and so they too remain undisclosed to the physician.
Amanda Marshall's award winning 2001 song "Everybody's got a story" reminds us that we can never assume that we have the whole story about a person. Her lyrics are a reminder not to "assume everything on the surface is what you see."
Hair loss is so closely tied in to a patient's self identity and how they feel about themselves. A key part of being a hair loss physician is understanding that there is so much more to losing hair than losing hair. There are a tremendous number of extremely complex emotions and psychological factors at play in anyone experiencing hair loss. Some of these factors are understood by the patient and shared openly. Othertimes these issues are understood by the patient and not shared openly. And other times yet they may not even be fully understood by the patient. Both of the latter two situations create a void in the physician's full understanding of their patients. And so we can never assume we understand the impact of any given patient's hair loss. However, assuming that it does matter to them is an assumption that works well for me.
When it comes to hair loss, everybody has a story to tell.
I posted an answer to a new question on Realself.com
I posted an answer to a new question on Realself.com
I posted an answer to a new question on Realself.com
I posted an answer to a new question on Realself.com
I posted an answer to a new question on Realself.com
"Trichotillomania" refers to a form of hair loss where an individual pulls their own hair. It can sometimes be simply a habit - especially in very young children. In adolescents, the diagnosis of trichotillomania may signify underlying psychological illness including depression, anxiety, and eating disorders.
Trichotillomania, alopecia areata and tinea capitis are the three most common diagnoses in children followed by telogen effluvium and androgenetic alopecia. One must always at least consider this diagnosis as it is easy to miss. The presence of broken hairs, black dots, hairs of different length, and other trichoscopic features a v-sign, tulip hairs, and exclamation hairs are helpful in arriving at the diagnosis. The picture shows numerous scattered broken hairs (see green dots) in a young child with trichotillomania.
I posted an answer to a new question on Realself.com
I posted an answer to a new question on Realself.com
I posted an answer to a new question on Realself.com
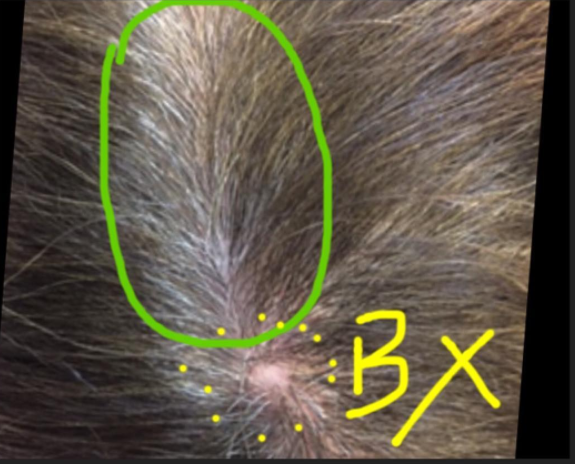
Scalp biopsies are helpful in situations where the diagnosis is not clear. If a biopsy needs to be performed, the sample should first and foremost be obtained from an area on the scalp that is most likely to display the histological features of the disease in question. However, one must also try to take a biopsy from an area that will hide any scar that may eventually form.
One of the easiest places to do a scalp biopsy is the central scalp right on the "central part line." This is rarely ever a good idea as the patient is likely to have a visible scar in the area for the rest of his or her life. Except in rare circumstances, there is usually no need to take a biopsy exactly on the central part.
A site 1-2 cm away from the area often serves equally well. If a biopsy must be taken from the central part, the patient should be warned about the potential for extreme visibility of the scar that will form in the area. The patient in this picture had a biopsy (BX) taken years ago from the central part (shown in green circle). The scar is obvious and regardless of the hairstyle chosen, it is challenging to hide.
I posted an answer to a new question on Realself.com