Prognosis of Folliculitis Decalvans: Pustules and Younger Age Associated with More Severe Disease
What Clinical Factors are Associated with More Severe Disease in Folliculitis Decalvans?
Vañó-Galván and colleagues recently retrospectively reviewed their data of 82 folliculitis decalvans patient in order to better understand associated clinical features and response to treatment.
Their study included patients from 12 dermatology centers across Spain. There were 82 patients (52 males and 30 females) with a mean age of 35 years. The vertex was the most common site. There were no significant comorbidities. A family history was present in three males. Itching, trichodynia, tufted hairs and pustules were part of the disease although they were not all consistently present. The table below (modified from the authors’ paper summarizes this data).
Comparisons of Males and Females Shows important Findings
What I liked about the authors’ paper was the fact they had a good number of female patients which allowed them to compare data from males and females. Males were more likely to be younger at the time of diagnosis, have pustules and have associated androgenetic alopecia. They were also more likely to have a family history.
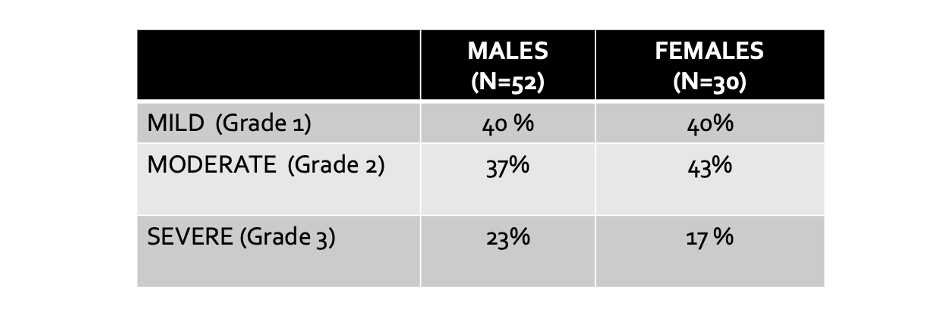
Other features were similar. The distribution of severity was similar in males and females as were the proportions of patients having symptoms like trichodynia and pruritus and the proportion showing clinical features liked tufted hairs.
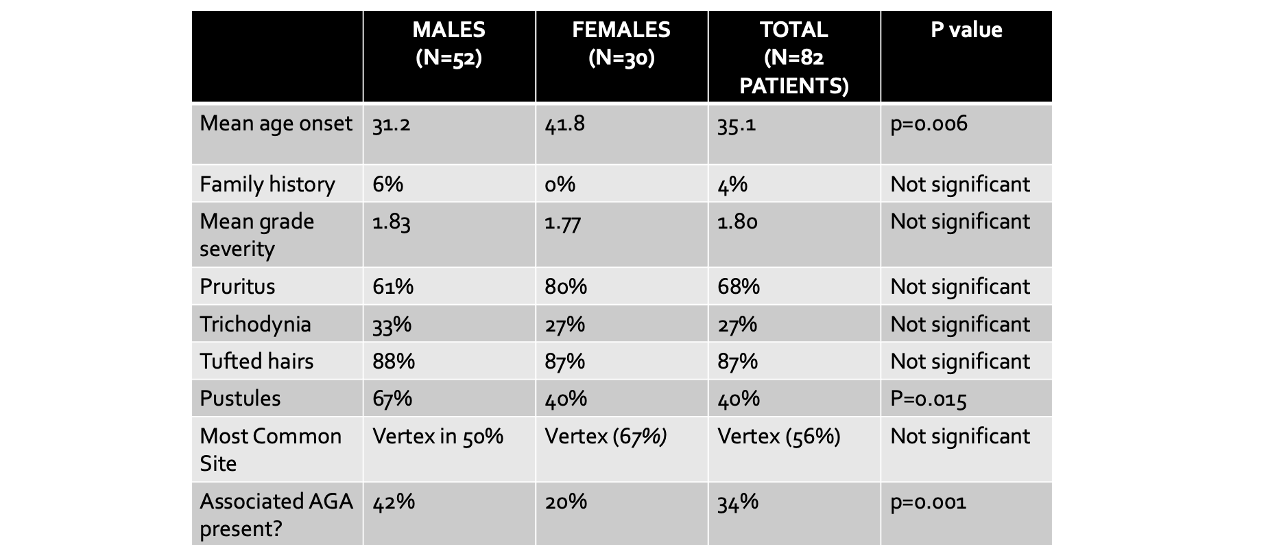
Modified from table in Vañó-Galván S et al. Folliculitis decalvans: a multicentre review of 82 patients. J Eur Acad Dermatol Venereol. 2015 Sep;29(9):1750-7.
Distribution of Severity Found to be Similar in Males and Females
Overall, 33 patients (40%) presented grade-I FD (largest patch less than 2 cm), 32 patients (39%) had grade-II FD (largest patch 2 to less than 5 cm) and 17 patients (21%) had grade-III FD (largest patch having a diameter of 5 cm or more,
Sites of Involvement: Vertex is Most Common Site in Males and Females
The most frequently affected area was the vertex (46 patients, 56%). Other affected areas included the parietal area (nine patients), the occipital area (five patients) and the frontal area (five patients).
In 69 patients (84%), there was just a single unique alopecic patch of hair loss that was detected. In 13 patients (16%), the patient presented with 2–5 alopecic patches. Eyebrow loss was noted in 5 patients and beard involvement was noted in one patient. Eyelashes and body hair were not involved in this study of FD.
Swab Culture Results
Bacterial cultures from the pustules of the patch of hair loss were obtained in 33 patients. A positive result was noted in 73% of cases. The isolated bacterium was S. aureus in all cases except one case (where it was E. cloacae). Nasal bacterial cultures were performed in 10 patients with a positive result in 100% of cases. S. aureus the isolated bacterium in all of the nasal swabs
Factors Associated with Severe FD
The authors explored factors that were associated with more severe FD. They found that two in particular stood out : onset of FD before 25 years of age and presence of pustules.
Onset of FD before 25 years of age was associated with a 12 fold increased risk of having severe disease (OR: 12.4; 95% CI 1.49–103.08; P = 0.020). The presence of pustules in the alopecic patch was associated with a four fold increased risk (OR: 3.94).
Treatment of FD: Oral Antibiotics, Steroid Injections, Isotretinoin Provide Options
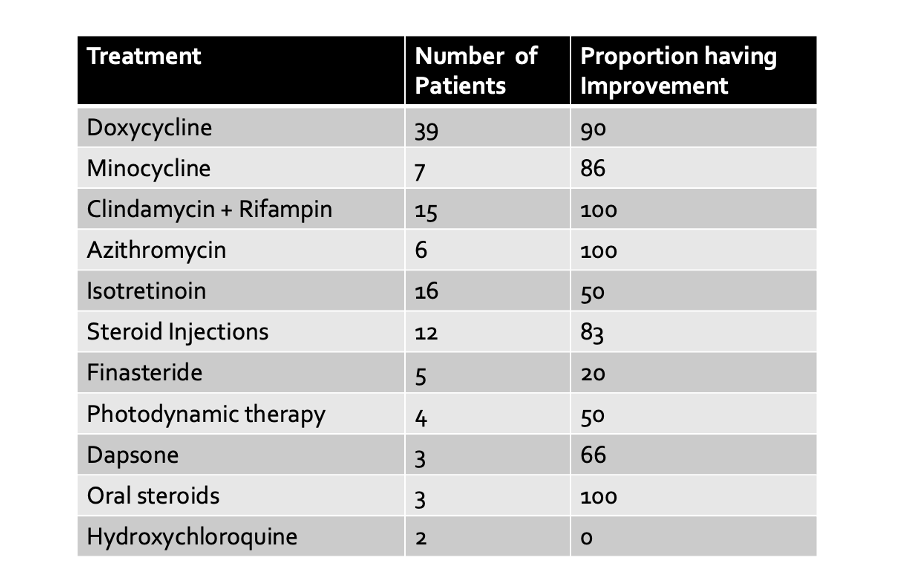
Oral antibiotics (particularly the tetracycline family and the combination of clindamycin and rifampicin) helped 90% and 100% of the patients, respectively. The authors’ full breakdown of treatment responses according to the drug chosen is shown in the Table below.
COMMENT
This is one of the largest retrospective studies of FD to date.
the vertex is the most common site in males and females. Males a re more likely to be diagnosed at an earlier age, have pustules and have associated AGA.
Yellow+younger are the two really important words not to miss here. Yellow refers to pustules in the alopecic patch and younger refers to age less than 25. These are the two independent factors associated with more severe disease.
The authors favour the use of antibiotics such as tetracycline family members (doxycycline, minocycline) the combination of clindamycin and rifampicin and dapsone are among the top options. Isotretinoin and steroid injections are very much on the list too
.
REFERENCE
Vañó-Galván S et al. Folliculitis decalvans: a multicentre review of 82 patients. J Eur Acad Dermatol Venereol. 2015 Sep;29(9):1750-7.
This article was written by Dr. Jeff Donovan, a Canadian and US board certified dermatologist specializing exclusively in hair loss.