Microblading for FFA Patients Using Isotretinoin
Is eyebrow microblading safe for FFA patients using isotretinoin?
I’ve selected this question below for this week’s question of the week. It allows us to review some concepts regarding isotretinoin and procedures for patients with FFA.
Question
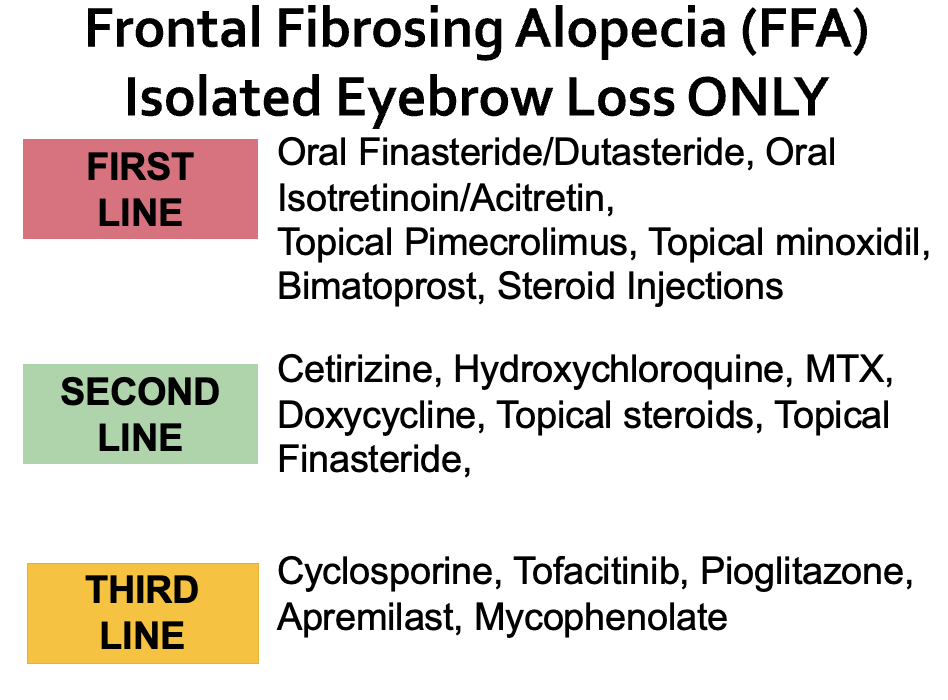
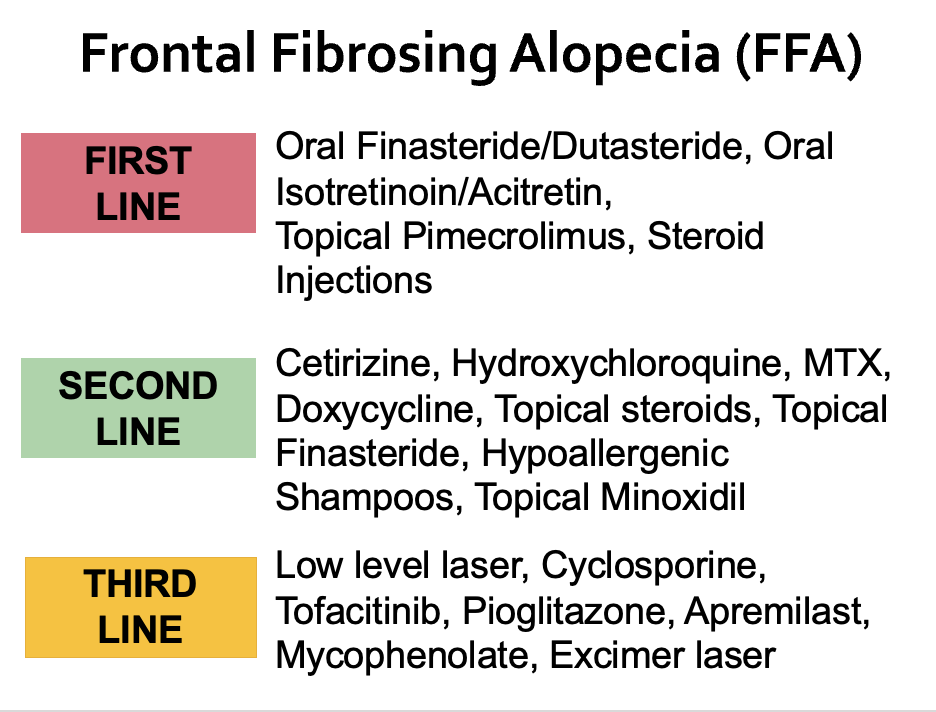
I am a 54 year old female with frontal fibrosing alopecia. Similar to many women, I have lost a significant amount of eyebrows. My scalp FFA has improved a great deal with use of dutasteride, isotretinoin, pimecrolimus and steroid injections. My eyebrow hair loss has halted but unfortunatley it has not grow back.
I am considering microblading for my eyebrows. The lady I see won’t do the microblading if I’m on isotretinoin and says I need to be off 6 months or more. Obviously, I am terrified to stop as it’s helped my scalp and facial bumps a very significant amount.
Should I stop the isotretinoin?
Thank you for your question section of the website so that we can ask questions of this kind.
Answer
Thanks for the great great question.
Isotretinoin is a vitamin A derivative and can affect many parts of the skin including the epidermis, sebaceous gland, and even collagen formation. The diverse affects of isotretinoin on wound healing have generated a long debate about whether patients who use isotretinoin are more likely to have poor wound healing or worse yet - develop a keloid or hypertrophic scar - if they undergo surgery or a procedure on the skin.
In fact, the US FDA advises against patients having laser resurfacing procedures within 6 months of use of isotretinoin.
The general recommendations to avoid surgical procedures have been called into question by various experts around the world in the last few years.
Tattooing in the Eyebrow Region in FFA
It appears that tattooing in the eyebrow area is likely to be safe in patients with FFA who use low doses of isotretinoin (under 10 mg daily). One should be aware that large scale studies have not yet been conducted in FFA but certainly we have had many stable patients in our clinic on low doses of isotretinoin undergo various tattooing procedures without issue.
For those who question the safety, a thorough review of two articles would be advised:
Spring et al, 2017
In 2017 a panel of experts (Spring et al 2017) put forth recommendations on the safety of isotretinoin in various dermatological procedures. Thirty-two relevant publications reported outcomes of 1485 procedures. Overall, the authors concluded that “there was insufficient evidence to support delaying manual dermabrasion, superficial chemical peels, cutaneous surgery, laser hair removal, and fractional ablative and nonablative laser procedures for patients currently receiving or having recently completed isotretinoin therapy. Based on the available literature, mechanical dermabrasion and fully ablative laser are not recommended in the setting of systemic isotretinoin treatment” (Source: Spring et al 2017).
Mysore et al, 2017
In 2017, the Association of Cutaneous Surgeons of India also put forth a recommendation “that microneedling and microdermabrasion treatment can safely be performed in patients administered with isotretinoin”. The level of evidence was 2+ (backed up by well conducted case control studies or cohort studies) and the grade of the recommendation was given a C rating.
The formal view of the Association of Cutaneous Surgeons of India was that “there is insufficient evidence to support the current protocol of avoiding and delaying treatments in the patient group under consideration and recommends that the current practice should be discontinued. The task force concludes that performing procedures such as laser hair removal, fractional lasers for aging and acne scarring, lasers for pigmented skin lesions, fractional radio-frequency microneedling, superficial and medium-depth peels, microdermabrasion, dermaroller, biopsies, radio-frequency ablation, and superficial excisions is safe in patients with concurrent or recent isotretinoin administration.
Conclusion and Comment
My general feeling is that tattooing of eyebrow is likely to be pretty safe for patients with FFA who use low doses of isotretinoin. We have not had problems with patients who use 10 mg daily or less AND whose FFA is fairly stable. I am not a big fan of eyebrow tattooing in patients with super active FFA simply because I have never guided patients through tattooing unless the FFA is somewhat calm. Likely tattooing is even active FFA is safe but of course no data is widely available. We also don’t have patients on higher doses of isotretinoin.
If one is willing to accept a really low risk of problems, then eyebrow tattooing is wonderful - assuming an experienced and competent practitioner is doing the tattooing. Close follow up with the dermatologist is advised so that immediate action can be taken in the event there are problems (ie. administration of topical steroids, steroid injections, topical calcineurin inhibitors). It is fortunately very rare to have problems other than the side effects that anyone experiences with tattooing. The improvement in self confidence and feeling of well being after successful tattooing procedures is great.
If a patient with FFA is not comfortable with any risk whatsoever, then eyebrow tattooing might not be the right procedure for them. At minimum, such a patient should be off isotretinoin for 6 months if they are not comfortable with risk - but again I must emphasize that this is without evidence and one risks worsening their scalp FFA if they stop isotretinoin and the isotretinoin was helping them.
Eyebrow microblading has its own inherent risks (even without isotretinoin!!) so all risks need to be reviewed with the practitioners performing the procedure. Persistent redness, tattoo reactions, bumps, poor uptake of pigment, rapid fading of pigment, allergic reactions are all part of the side effects for anyone with or without FFA. One should never undergo tattooing without first reviewing what sorts of rare side effects occur in anyone.
Finally, one must be aware that pigments don’t always taken up quite as well in FFA. The skin is different in some patients and takes of pigments differently - so multiple procedures may be needed. One must never ever assume that the microblading outcome they will have will necessarily be the same as anyone else who does not have FFA. The skin is different and it’s possible for variations in outcomes.
Fortunately, most patients have really nice results and the vast majority of patients are really pleased with the decision to have microblading and other pigmentation procedures. One should carefully review the risks and benefits with the dermatologist overseeing care as well as the tattoo expert performing the procedure. A full understanding of risks and benefits is needed.
REFERENCE
Mysore V et al. Standard Guidelines of Care: Performing Procedures in Patients on or Recently Administered with Isotretinoin J Cutan Aesthet Surg. 2017 Oct-Dec; 10(4): 186–194.
Spring L et al. Isotretinoin and Timing of Procedural Interventions: A Systematic Review With Consensus Recommendations. JAMA Dermatol . 2017 Aug 1;153(8):802-809.