Atrophy (Indentations) from Scalp Steroid Injections: Should I be Stopping?
Scalp Indents (Atrophy) from Steroid Injections: What should I be doing?
Steroid injections are generally well tolerated and have a good safety profile for most when the correct concentration and dose are used. Atrophy or small indentations or depressions in the skin are side effects that can sometimes occur with steroid injections. They are temporary in nature but it is important that one does not continue to inject in the area if atrophy is present. Injections of the depressed area with saline (salt water) often speeds up the resolution - possibly by stimulating the scalp to make collagen, Injections need to be postponed in the area of atrophy if indentations are noted. Once the scalp improves back to normal in that area we can often continue the injections.
Atrophy can often resolve on its own but may take 2-5 months to do so. The speed and completeness of resolution depends on several factors including 1) if injections were performed in areas that already had atrophy as well as 2) how much “topical” steroid is being used while the atrophy is trying to improve as well as 3) the concentration of steroid injected and 4) intrinsic characteristics of the disease itself and the skin of the patient. Not all patients experience total resolution but most do if steroids are reduced or abandoned during the process.
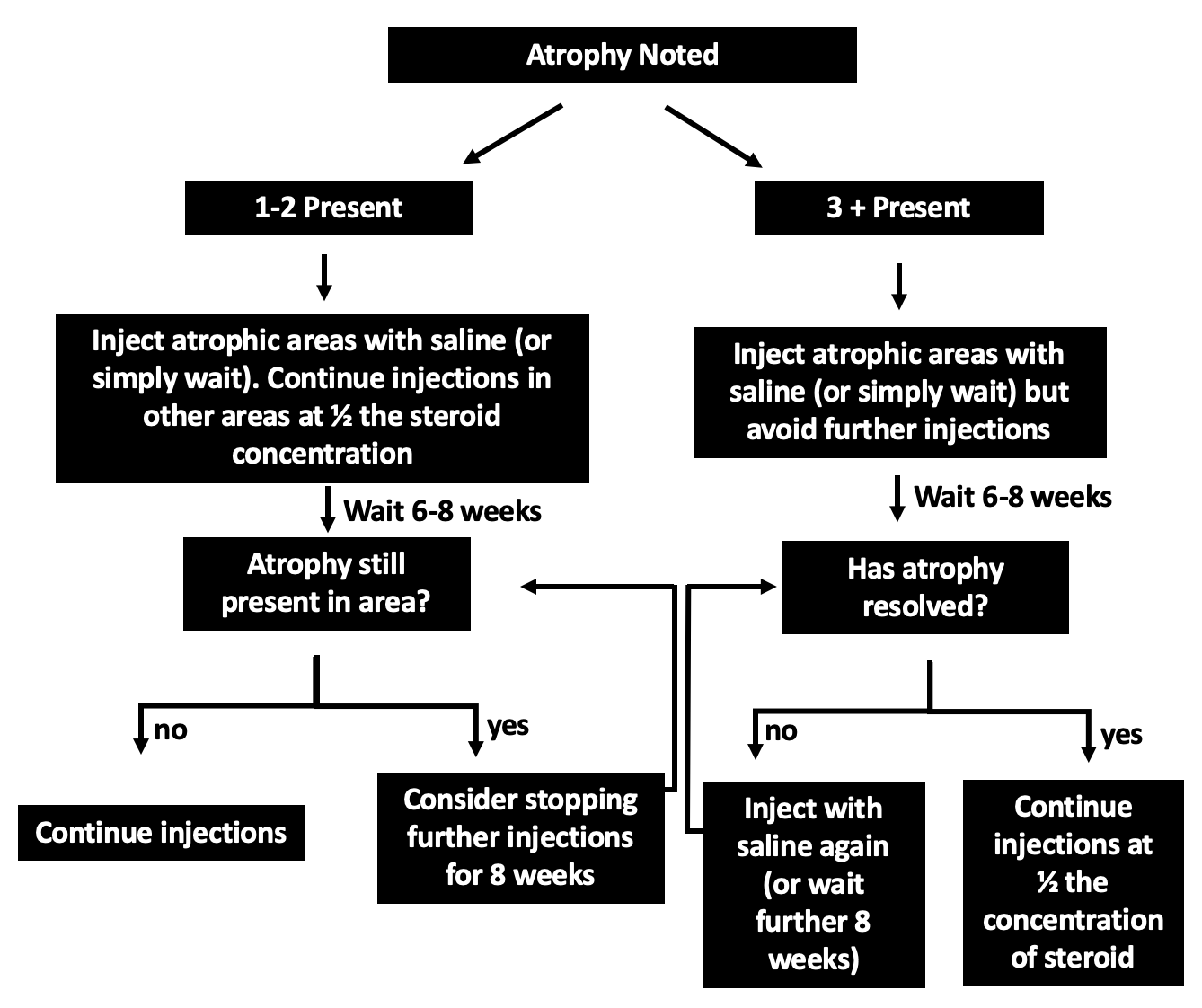
The presence of atrophy does not mean that injections need to be stopped altogether only but do indicate that injections need to be stopped in the area of atrophy. If there are only 1-2 indentations, then it may be possible to simply avoid injections and continue injections in other areas that require injections (at a lower dose). If there are 3 or more indentations, I recommend waiting 6-8 weeks to have the skin improve before attempting injections again. When injections are restarted, I recommend that a lower dose be used.
The Dose of Triamcinolone acetonide (Kenalog)
One must always consider the dose of steroid that was used. Some physicians use 10 mg per mL which has a higher chance of causing atrophy than 5 mg per mL. Some physicians use 2.5 mg per mL or 3.3 mg per ML which are both common doses that I use in many patients. A patient who gets atrophy from 10 mg per mL might still benefit from 2.5 mg per mL and so steroid injections need not necessarily be totally abandoned. Of course this is handled on a case by case basis.
For any patient with atrophy, one must also consider just how much topical steroid is being used. A patient who is using extremely large amounts of high potency topical steroids may be more likely to get atrophy if injections are then performed as well.
Above is my algorithm for dealing with atrophy from steroid injections.
This article was written by Dr. Jeff Donovan, a Canadian and US board certified dermatologist specializing exclusively in hair loss.