Desmoplastic Melanoma Mimicking Alopecia Areata
Case of Desmoplastic Melanoma Has Important Lessons for the Hair Loss Practitioner.
A new report in JAAD Case Reports highlights the case of a patient with desmoplastic melanoma (DM) that could be easily mistaken for alopecia areata. Fortunately, brilliant steps taken by the dermatology team allowed the correct diagnosis to be determined and treatment initiated.
Desmoplastic melanoma (DM) is a rare spindle cell variant of melanoma, accounting for only 1% to 4% of cutaneous melanomas. It occurs slightly more often in males than females (M:F ratio 2:1) and the mean age of onset is 66 years. The authors remind us that early diagnosis is often challenging with these types of melanomas because they are amelanotic. They often appear as indurated poorly demarcated plaques.
CASE
The case the authors present is that of a 43 year old male with a history of pilar cysts in the past who now presents with a 3x2 cm new patch of hair loss in the right frontal scalp. The area of hair loss was in an area which previously had pilar cysts and had previously received surgical treatment for those pilar cysts. The area of hair loss was present for several months. The area was treated by the primary care provider with fluocinonide 0.05 % topical solution but the hair did not grow back. The patient was then referred to a dermatologist.
Two punch biopsies were obtained on the right central frontal scalp and the pathologist confirmed the diagnosis of desmoplastic melanoma.

Figure 1 from the article by LaMonica et al showing an area of hair loss that was refractory to treatment with topical steroids. Biopsy of the area subsequently showed a desmoplastic melanoma. FROM: LaMonica LC et al. Desmoplastic melanoma presenting as an alopecic patch in a young patient. JAAD Case Rep. 2023 Aug; 38: 96–99. Image used with creative commons license.
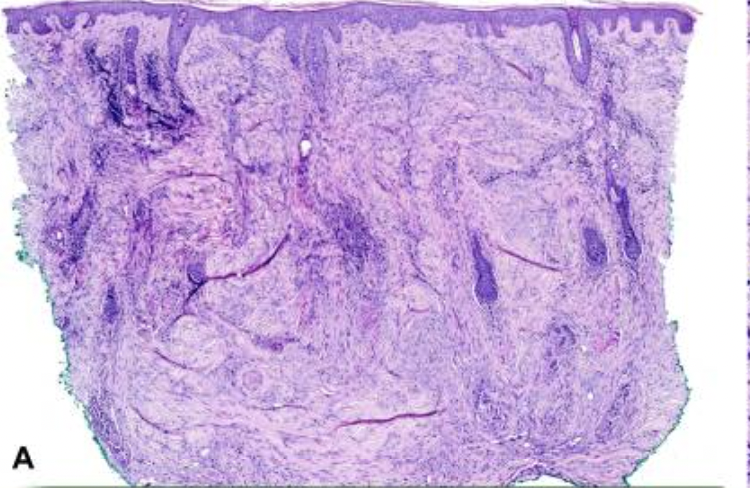
Figure 2A from the paper by LaMonica et al showing histopathological findings from a vertically sectioned punch biopsy. The specimen shows a dense spindle cell proliferation with associated desmoplastic stroma. FROM: LaMonica LC et al. Desmoplastic melanoma presenting as an alopecic patch in a young patient. JAAD Case Rep. 2023 Aug; 38: 96–99. Image used with creative commons license.

Figure 2B from the paper by LaMonica et al showing atypical spindle cells with hyperchromatic, pleomorphic nuclei and associated desmoplastic stroma. FROM: LaMonica LC et al. Desmoplastic melanoma presenting as an alopecic patch in a young patient. JAAD Case Rep. 2023 Aug; 38: 96–99. Image used with creative commons license.
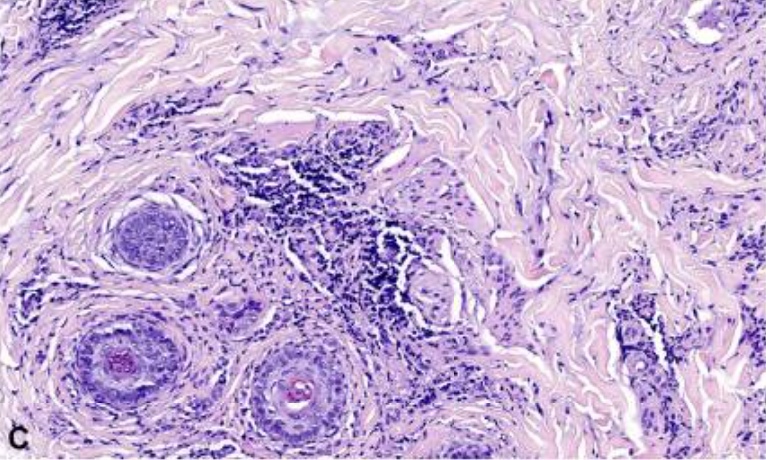
Figure 2C from the paper by LaMonica et al showing follicular miniaturization and obliteration of hairs by the atypical spindle cell neoplasm. There is an associated desmoplastic stroma and brisk lymphocytic infiltrate. FROM: LaMonica LC et al. Desmoplastic melanoma presenting as an alopecic patch in a young patient. JAAD Case Rep. 2023 Aug; 38: 96–99. Image used with creative commons license.
The patient was then immediately referred for wide local excision. A full-thickness donor graft from the right supraclavicular region was used for closure. A sentinel lymph node biopsy of 2 right neck lymph nodes was performed and was negative for malignant spread. Evaluation of the excisional specimen revealed a final tumor depth of 8.0 mm with final pathologic staging of IIB (pT4aN0m).
Discussion
This is a very interesting case. It’s incredible that such timely diagnosis came about. The case has such important lessons for all of us: if a patch of presumed alopecia areata does not seem to be growing back, the clinician needs to at least have in the back of his or her mind the possibility that this may not be alopecia areata.
Now, not every patch of alopecia areata is going to grow with topical steroid and we can’t be biopsying every patch of alopecia areata that fails to grow back. However, patches that are bumpy or irregularly shaped or fibrotic or red or studded with nodular or papular lesions may need a biopsy. In addition, alopecia areata like lesions that don’t show typical signs of exclamation mark hairs or yellow dots or broken dots may raise suspicion that something is wrong.
This was really a great case presentation. What makes this case so interesting is that the patient had a history of pilar cysts in the area which had been surgically treated. If you’ve ever seen a scalp with previously treated pilar cysts you realize that sometimes it does not turn out so cosmetically perfect. There is hair loss and irregularities to the scalp (hopefully minor). It would be easy to attribute this patient’s hair loss to pilar cysts or a complication of prior surgery. It was the astute physician who did a biopsy that allowed this cancer to be diagnosed at the earliest possible stage.
The authors remind us that “alopecia neoplastica” is a phenomenon whereby neoplastic cells and accompanying fibrosis replace/obliterate hair follicles. Most cases of AN are “secondary” to visceral cancers from the gastrointestinal tract, breast, kidney, and lung. The authors note that true “primary” AN is less common but incledes primary malignant neoplasms such as angiosarcomas, hemangioendotheliomas, ectopic extramammary Paget disease, syringomatous carcinoma, amelanotic melanoma, and desmoplastic melanoma.

The authors remind us that there have been 4 cases in the literature with “SCAR-LIKE PATCHY ALOPECIA.” Some cases were red. Some resembled alopecia areata, discoid systemic lupus erythematosus, and lichen planus. References for these cases are shown below in the reference section.
Alopecia Neoplastica should be considered in patients presenting with an unusual scarring alopecia like presentation or with an alopecia areata like presentation that fails to respond to treatment

REFERENCE
LaMonica LC et al. Desmoplastic melanoma presenting as an alopecic patch in a young patient. JAAD Case Rep. 2023 Aug; 38: 96–99.
Crotty K., McCarthy W., Quinn M., McCarthy S. Alopecia neoplastica caused by desmoplastic melanoma. Australas J Dermatol. 2003;44(4):295–298. doi: 10.1046/j.1440-0960.2003.00013.x.
Erstine E.M., Elwood H.R., Westbrook K.C., McCalmont T.H., Shalin S.C., Gardner J.M. Desmoplastic melanoma presenting as primary alopecia neoplastica: a report of two cases. J Cutan Pathol. 2016;43(10):872–879. doi: 10.1111/cup.12758.
Furlan G.L., Bortolozzo M.B., Moura K.C., Petrarolha S.M.P., Dedivitis R.A. Desmoplastic melanoma. Arch Head Neck Surg. 2020;49 doi: 10.4322/ahns.2020.0006.
This article was written by Dr. Jeff Donovan, a Canadian and US board certified dermatologist specializing exclusively in hair loss.