Does my Patient have Lichen Planopilaris with AGA or Fibrosing Alopecia in a Pattern Distribution?
LPP + AGA vs FAPD: What’s the better term for my patient ?
Today, I will speak briefly on the topic of fibrosing alopecia in a pattern distribution or “FAPD” and more broadly on the topic of fibrosing alopecias.
FAPD is viewed as a type of lichen planopilaris whereby the immune system of affected patients is preferentially targeting miniaturizing and vellus hairs. The term FAPD is often incorrectly applied to situations whereby the patient is noted to have both androgenetic alopecia and lichen planopilaris. This is not correct. FAPD is actually a distinct entity that has overlapping features of AGA and LPP but is not a term that should be given to every patient who is found to have both AGA and LPP. About 50% or more of patients with LPP will have features of AGA - however only a small proportion of patients have FAPD.
I view FAPD as aa condition where the immune system really cares about attacking the miniaturizing hairs. I view LPP as a condition whereby the immune system focuses on attacking all types of hairs with less specific focus on miniaturizing hairs.
The Zinkernagel and Trüeb 2000 Study
Physicians who are going to use the term FAPD and write it down somewhere in a patient’s chart need to understand the Zinkernagel and Trüeb 2000 study really well. The term fibrosing alopecia in a pattern distribution (FAPD) was first introduced by Zinkernagel and Trüeb in 2000. The authors of this 2000 study described 19 patients who presented with hair loss showing features of both androgenetic alopecia and lichen planopilaris. However, the well-defined scarred areas that are typically seen in classic LPP were not present.
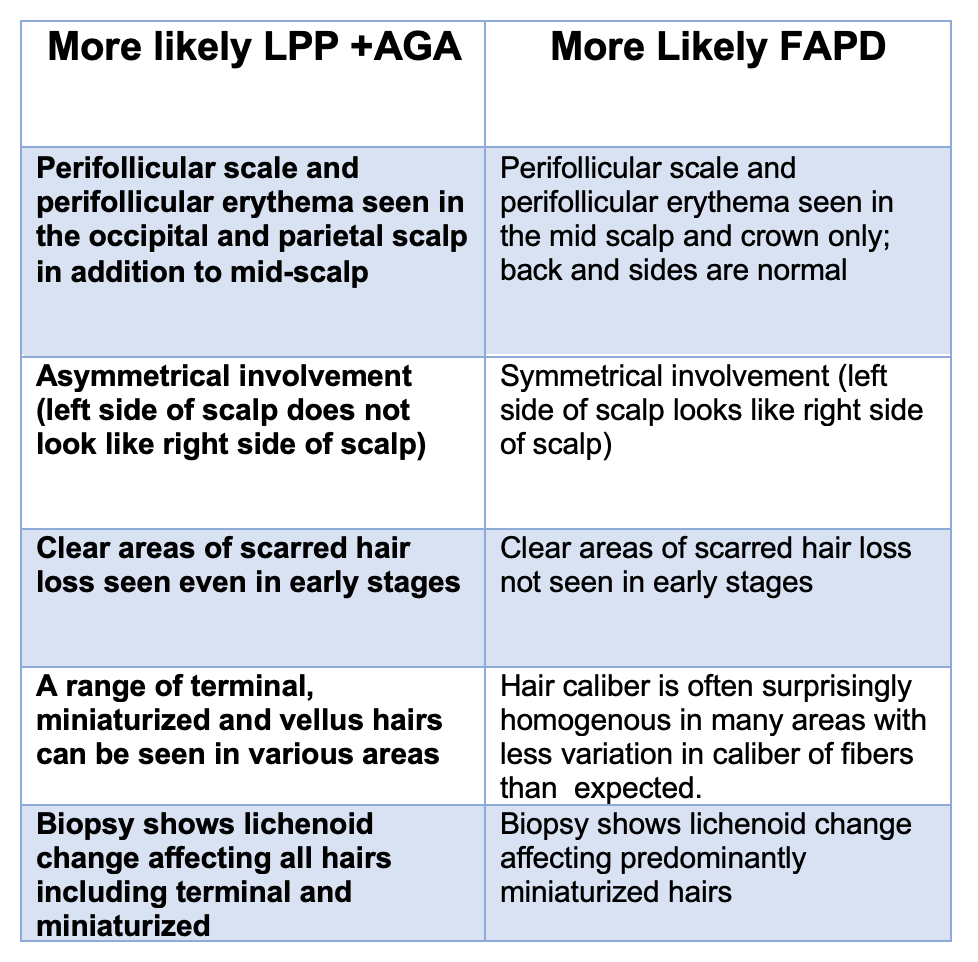
Patients with FAPD first appear to have androgenetic alopecia with redness that is often mistaken for seborrheic dermatitis. Of course, seborrheic dermatitis may also be present given that it is a common condition. However, a closer look shows that there is perifollicular erythema and sometimes also perifollicular scale. The key in FAPD is that this inflammation is predominantly targeting the miniaturizing hairs.
Not all patients with FAPD have symptoms. In fact, only 37 % of patients with FAPD in the Zinkernagel and Trüeb study had symptoms of itching or pain. However, all patients showed perifollicular erythema on trichoscopy and 79 % of patients showed loss of the follicular openings. 58 % showed perifollicular scaling in the area of hair loss. However, all patient biopsies in the Zinkernagel and Trüeb study showed features of lichen planopilaris. Of 14 patients in the Zinkernagel and Trueb study that underwent biopsy, 100% had a perifollicular lymphocytic infiltrate, 93 % had 57 % had perifollicular fibrosis, 57 % had follicular interface dermatitis, 29 % showed keratinocyte necrosis and 71 % showed hair follicle miniaturization.
Treatments for FAPD include antiandrogens, clobetasol and minoxidil. Treatments for FAPD include antiandrogens, clobetasol and minoxidil. Antiandrogens not only address the androgenetic hair loss but have been found to reduce inflammation in some patients with FAPD. Antiandrogens are less helpful in treating classic LPP unless of course AGA is also present. Antiandrogens are generally quite helpful in FAPD
A Brief Word about the “Fibrosing Alopecias”
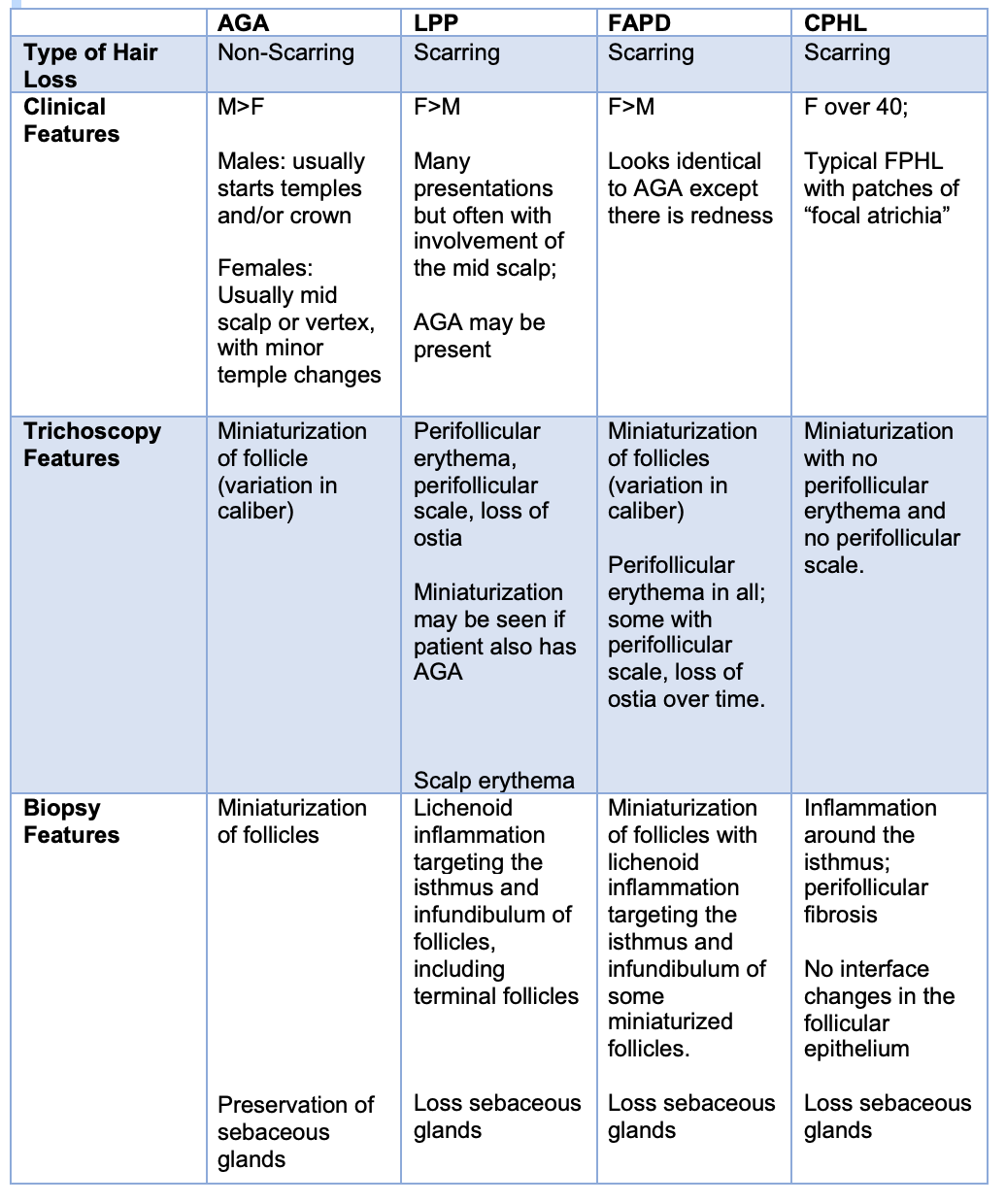
There is a new term popping up in the medical literature referring to scarring alopecias that share similar features. Classic Lichen planopilaris, Fibrosing Alopecia in a Pattern Distribution, Cicatricial Pattern Hair Loss, Frontal Fibrosing Alopecia and Central Centrifugal Cicatricial Alopecia all belong to this group of fibrosing alopecias.
The most challenging clinically to sometimes distinguish are classic LPP from FAPD and Cicatricial Pattern Hair Loss. Both LPP and FAPD show changes in the follicular epithelium by biopsy (keratinocyte necrosis, lichenoid change). Sometimes, of course, these changes are not caught on biopsy. CPHL is a form of AGA which does not show changes in the follicular epithelium on biopsy The following table helps clinical differentiate between these conditions.
This article was written by Dr. Jeff Donovan, a Canadian and US board certified dermatologist specializing exclusively in hair loss.