Loose Anagen Hair Syndrome.
Loose Anagen Hair Syndrome is Typically Seen in Young Children
Loose anagen hair syndrome (LAHS) is not a very common hair loss condition. however, unless one is thinking about this condition as they evaluate a patient - the diagnosis is likely to be easily missed. The key finding of LAHS is the ability to painlessly and effortlessly remove abnormally appearing anagen hairs from the scalp.
The typical patient who comes to see me with a diagnosis of LAHS is a healthy, fair-haired girl age 3-6. The parents who accompany the patient raise concerns about many issues including such issues as the hair "does not grow long" or "rarely needs to be cut" or is “easily pulled out” by siblings or friends. Girls with the syndrome predominate over boys (6:1 to 36:1), and patients with blond and light brown hair predominate over those with dark-colored hair.
Although onset is typically in younger ages (3-6), a range of ages can be seen, including adults.
What’s the cause of LAHS?
The exact cause remains unknown. There is defective anchoring of anagen hairs which causes them to be easily and painlessly extracted from the scalp. The defective anchoring occurs due to abnormal adhesion between the hair shaft and the inner root sheath (IRS). It is thought that there is abnormal premature keratinization of the IRS that impairs the adhesion between the cuticle of the IRS and the cuticle of the hair shaft. In addition, defective adhesion between the outer root sheath and inner root sheath may also contribute in some patients.
In addition to a defective cohesion, Dr Price and colleagues proposed that the anagen duration is less which accounts for shorter growing hairs in some patients.
LAHS is usually an isolated phenomenon occurring in healthy children with normal growth and development. However, the syndrome has been reported in association with several hereditary and developmental disorders including Noonan-like syndrome, ocular coloboma syndrome, trichorhinophalangeal syndrome, alopecia areata, nail patella syndrome, hypohidrotic ectodermal dysplasia, ectrodactyly-ectodermal dysplasia clefting syndrome, acquired immunodeficiency syndrome, diffuse partial wooly hair syndrome, colobomas with dysmorphic facial features, uncombable hair syndrome and neurofibromatosis. It is possible that some of these associations are coincidental. However, for some, such as Noonan-like syndrome with loose anagen hair, specific gene mutations (i.e. SHOC2) have been consistently identified in affected patients.
The Three Patterns of LAHS
According to Dr. Elise Olsen and her colleagues, concerns about hair may follow 3 patterns in LAHS :
TYPE A PRESENTATION: hair that is thin, sparse and fine
TYPE B PRESENTATION: hair that is unmanageable and unruly
TYPE C PRESENTATION: hair that is shedding
The type A and type B presentations are most commonly seen in children with LAHS, and might even evolve into the C type as children age. The type C presentation is most commonly seen in adults.
What is seen on hair and scalp examination?
Patients with LAHS have a spectrum of findings on examination. There is not one classical presentation.
The hair density may be reduced, either diffusely or in localized (“patchy”) areas of the scalp. Completely bald areas, however, are never a feature of this syndrome. The vertex and occipital scalp are frequent areas of hair loss. Hair in the occiput may also be noted to be rough and sticky, and not lie flat. The distal ends of the hairs may be found to be of uneven lengths and lack shine. Lustreless hair is often reported by parents. There is no scalp inflammation or scarring seen on examination. The eyebrows, eyelashes and body hair are typically normal. There is no hair fragility on examination and no hair breakage. The teeth, nails and skin are normal.
Findings of The Pull Test
The key to the diagnosis of LAHS is the ability to easily remove “abnormal anagen hairs” with gentle traction when doing a so called “pull test.” Chapman showed that the amount of force required to pluck single scalp hairs in patients with LAHS is 3.4 times less than in patients who do not have this condition. Specifically, the authors showed a mean value of 14 g compared to 48 g for normal controls.
A pull test of 50 hairs shows that hairs can be easily removed without effort. When these hairs and then examined under the microscope, a patient with LAHS will have about 10 hairs extracted that fit the definition of LAHs.
A few points about the pull test are important:
[1] It’s important to realize that as hair follicle of a typical LAH goes through its normal hair cycle, there will be time where the hair is better glued into the scalp the other times. Therefore a negative hair pull test does not exclude LAS and a trichogram is essential to confirm the diagnosis if the pull test is negative and suspicions for LAHS are high.
[2] The finding of loose anagen hairs (LAHs) when doing a pull test does not mean the patient has LAHS. Even healthy individuals can have some LAHs and patents with alopecia areata can have LAHs too.
In general, most children without LAHS have either no LAHs seen on the pull test or only 1 or 2 so the actual number is very important with considering rendering a diagnosis of LAHS. The diagnosis of LAHS depends on the percentage of abnormal LAHs that are seen on the pull test (or found on the trichogram). When doing the pull test, most authors feel that at least 10 of the 50 hairs must be LAHs.
Findings of the Trichogram
There are fewer and fewer physicians around anymore who perform “trichograms.” I do them from time to time but they are more frequently done by my European colleagues. A trichogram involves grasping 40 hairs with rubber lined epilating forceps and applying a 90 degrees rotating motion to get hairs out. Patients with LAHS have more than 50 % LAHs when the hairs from a trichogram are analyzed. Some set the cut off at 70% or 80 %. Tosti originally set the definition at 80 % in 1997 and then revised it to 70 % in 2002. in 2009, Cantatore-Francis and Orlow proposed a cut off of 50 %.
There are few telogen hairs seen in the trichogram of patients with LAHS.
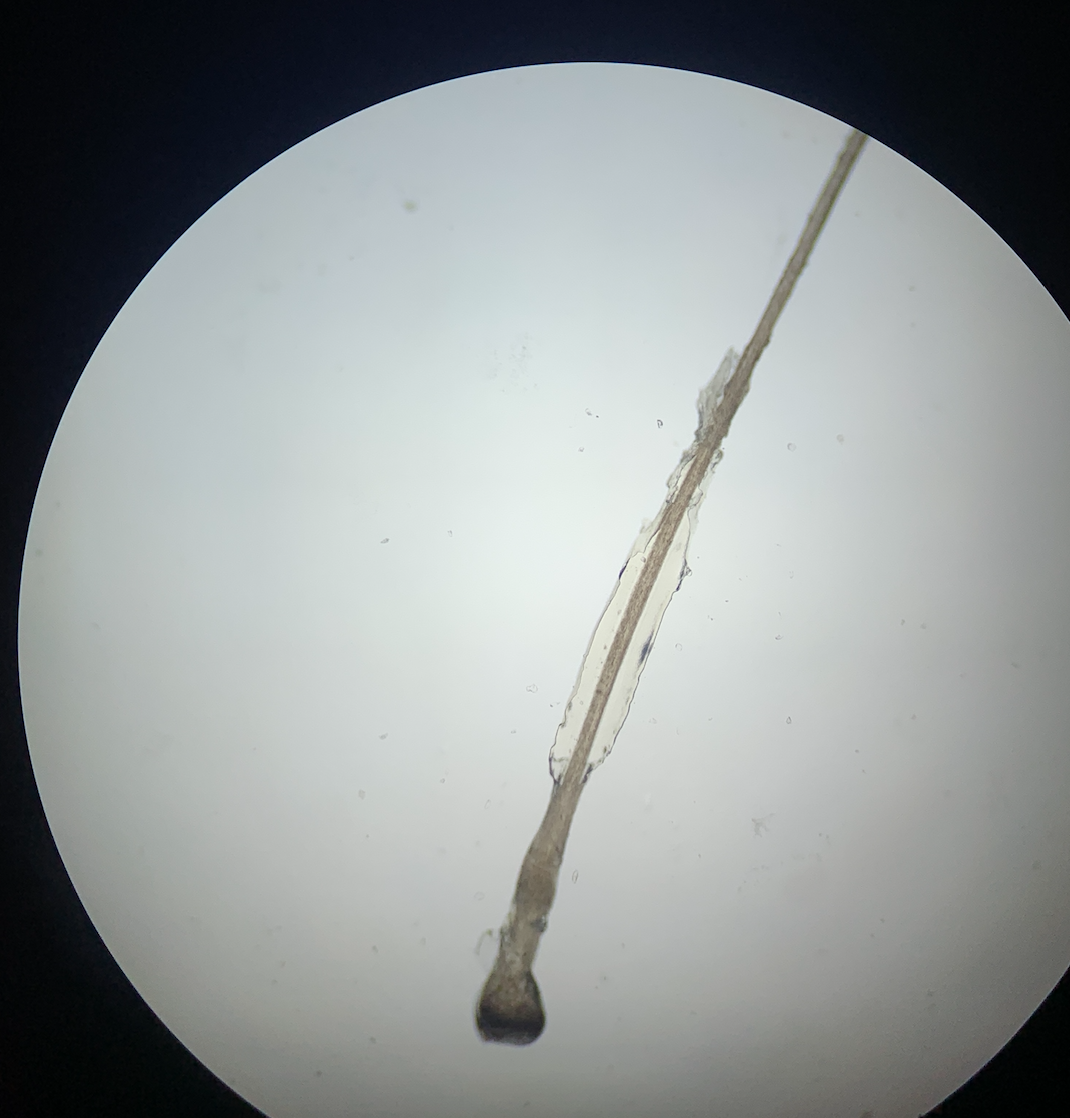
Loose Anagen Hairs (LAHs) What do the hairs look like anyways?
The morphology of the extracted anagen hairs is abnormal. The hairs may show misshapen bulbs. The cuticle may be ruffled. By light microscopy, the extracted anagen hairs lack both the internal and external root sheath and show a ruffled cuticle distal to the hair bulb. The appearance of the ruffled cuticle resembles a 'crumpled sock' that falls down around one's ankles. The appearance of the hair shaft resembles a 'golf club' or ‘mouse tail’ because the hair bulb frequently appears at an acute angle to the hair shaft rather than at the normal angle of 180 degrees.
Scalp biopsies and electron microscopy is not required for the diagnosis of loose anagen hair syndrome. H&E stained biopsy samples will show clefting between IRS, IRS and ORS, ORS and fibrous sheath. There is a lack of inflammation in LAHS. The presence of peribulbar lymphocytes suggests a diagnosis of alopecia areata rather than LAHs. The is important to note because there are reports (ie Nunez et al 1999) of patients with diffuse hair loss who had trichograms shows LAHs who actually had a diagnosis of alopecia. For this reason, a scalp biopsy should be at least considered in patient with LAHS. For children, this will likely not be done, but certainly for older children and adults suspected of having LAHs this is important.
Electron miscopy is rarely done for LAHS but will show that a proportion of the hair shafts have an abnormal shape with grooves, ridges and twisting. This leads to irregularly shaped hairs on cross-section.
Normal anagen hair from a patient without Loose Anagen Hair Syndrome.

Ruffled cuticle from a patient with LAHS

Abnormal Anagen Hair From LAHS: crumpled cuticle is seen
How do we treat LAHS?
It’s still not clear how best to treat LAHS. Fortunately, many children outgrow the condition and the anagen hairs in some individuals start to acquire a normal appearance. I usually advise parents that by age 10, many children will report very significant improvements. Some patients, however, do continue to have easily extractable hair into adolescence and adulthood.
Patients are advised to be as gentle as possible when shampooing the hair and grooming the hair in order to avoid extracting too many hairs. I also recommend that patients avoid using traumatic hair care practices, such as excessive braiding. Wearing the hair as naturally as possible may help the most.
The use of topical minoxidil is the most commonly used treatment in the management of LAHS. It may help some individuals speed up resolution. Minoxidil does not help all individuals with LAHS.
Reference
Cantatore-Francis JL, Orlow SJ. Practical guidelines for evaluation of loose anagen hair syndrome. Arch Dermatol. 2009 Oct; 145(10):1123-8.
Chapman DM, Miller RA. An objective measurement of the anchoring strength of anagen hair in an adult with the loose anagen syndrome. J Cutan Pathol. 1996;23:288–92.
Donovan J. Loose Anagen Hair Syndrome.
Nunez J, Grande K, Hsu S. Alopecia areata with features of loose anagen hair. Pediatr Dermatol. 1999 Nov-Dec; 16(6):460-2.
Olsen EA, Bettencourt MS, Coté NL. The presence of loose anagen hairs obtained by hair pull in the normal population. J Investig Dermatol Symp Proc. 1999 Dec; 4(3):258-60.
Price VH, Gummer CL. Loose anagen syndrome.J Am Acad Dermatol. 1989 Feb; 20(2 Pt 1):249-56.
Tosti A, Piraccini BM. Loose anagen hair syndrome and loose anagen hair Arch Dermatol. 2002 Apr; 138(4):521-2.
Tosti A, Peluso AM, Misciali C, Venturo N, Patrizi A, Fanti PA. Loose anagen hair. Arch Dermatol. 1997 Sep; 133(9):1089-93.
This article was written by Dr. Jeff Donovan, a Canadian and US board certified dermatologist specializing exclusively in hair loss.