Can oral minoxidil be safely used in patients with hypertension or arrhythmia?
Oral minoxidil can be used safely used in most patients with hypertension or arrhythmia
A new study set out to evaluate the safety of LDOM in patients with hypertension or arrhythmia. This was the first of its kind to examine the safety of LDOM in patients with HT or arrhythmia.
The study was a retrospective multicenter study of patients with hypertension or arrhythmia treated with LDOM for any type of alopecia. Patients were those under treatment with LDOM for hair loss of any cause for at least one month, at five centers from Brazil and Spain.
Patients with Hypertension
There were 254 patients with hypertension in the study. This included 176 women (69.3%) and 78 men (30.7%)]. The mean age of 56.9 years (range 19-82).
Although there was 254 patients, some patients were able to increase their LDOM doses so there was 382 doses. Patients were receiving between 0 and 5 antihypertensive drugs (mean 1.45) The most frequent drug class was angiotensin II receptor blockers (ARBs) in 190 patients (49.7%), followed by thiazides (28.5%), beta- blockers (28%), ACE inhibitors (19.6%), calcium channel blockers (16.4%), spironolactone (6.5%) , hydralazine (1.4 %) and doxazocin (0.7%).
58.9% of patients were using one blood pressure drug. 32.7% were on 2 drugs, 7.1 % were on 3 or more. 1.3 % were on no medications for blood pressure at all.
The mean dose of LDOM was 1.59 mg (range 0.2-10) and the mean duration was 10.9 months (range 1-51). Patients in this study have many different types of hair loss including androgenetic alopecia (68.9%), followed by frontal fibrosing alopecia (10.2%), telogen effluvium (4.3%), lichen planopilaris (3.5%), fibrosing alopecia in a pattern distribution (3.1%), alopecia areata (2.4%).
All in all, systemic side effects were detected in 6.8% of cases (26 cases total). This included lightheadedness (3.1%), fluid retention (2.6%), general malaise (0.8%), tachycardia (0.8%) and headache (0.5%). LDOM needed be stopped in 6 cases (1.5%).
All of the side effects improved with dose adjustment or stopping of the drug, and no life-threatening side effects were observed.
What were the factors predicting the need to stop LDOM?
Patients who received 3 or more antihypertensive drugs and those using doxazocin (an alpha an alpha-adrenergic blocker that also causes arteriolar vasodilation) were more likely to need to stop their drug.
In fact, patients who received 3 or more antihypertensive drugs had a higher risk of developing more than 1 side effect (P < 0.001), lightheadedness (P < 0.001), general malaise (P < 0.001) in addition to requiring LDOM discontinuation (P=0.012).
Also, prior treatment with doxazosin was associated with not only a higher risk of needing to stop LDOM (P < 0.001) but a higher risk of lightheadedness (P < 0.001), general malaise (P < 0.001), fluid retention (P = 0.01) and necessity of both dose adjustment (P = 0.006).
Comparison of Side Effects in Hypertensive Patients to General Population
The authors compare their data in their hypertensive group to the data from their 2021 study of 1400 patients. Side effects were fairly similar for the most part. However there was a slightly higher incidence of systemic side effects, light-headedness, fluid retention in those with hypertension.
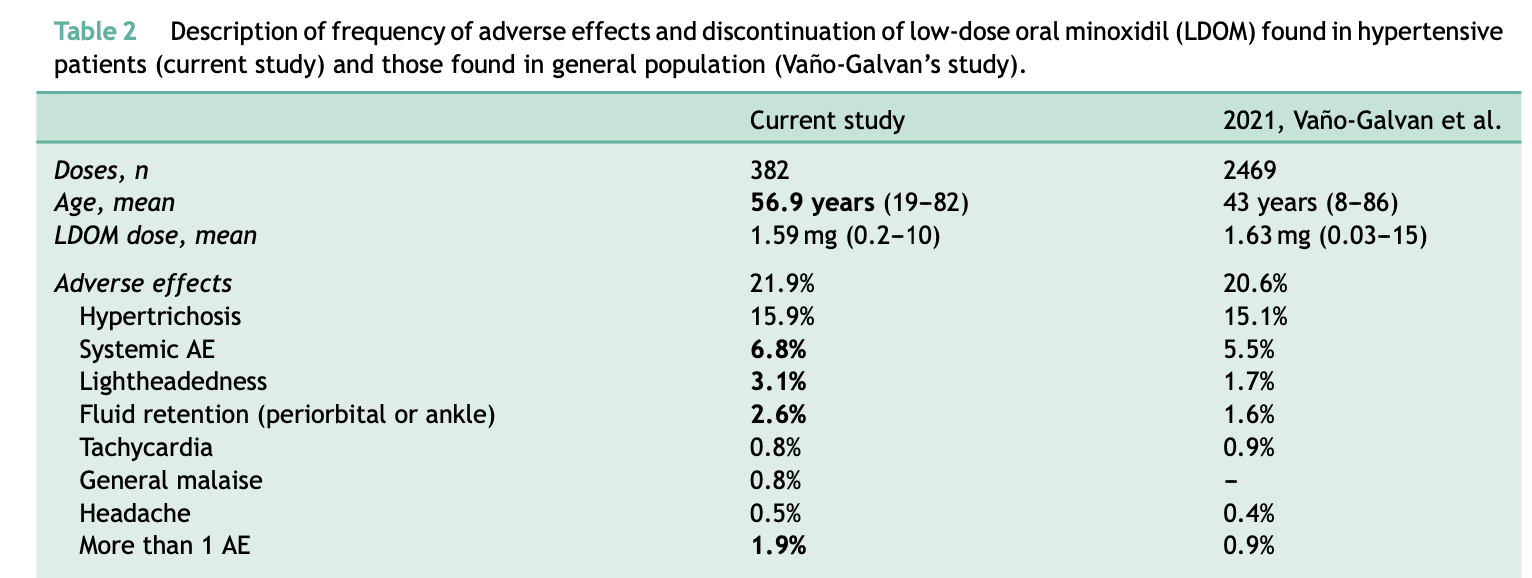
Comparison of Side Effects in Hypertensive Patients Compared to General Population. Used with creative commons license.
LDOM in Patients with Arrhythmia
Nine patients had personal history of arrhythmia, namely supraventricular extrasystole (n=3), atrial fibrillation (n = 1), sinus tachycardia (n = 1), cardiac syncope (n = 1), and unknown arrhythmia (n = 3, missing data).
From them, four patients were under medical treatment with beta- blockers (n=3) or amiodarone (n=1). Two patients had prior cardiac ablation and one patient had a pacemaker. Two patients were not currently receiving any treatment. The remaining patient had a mechanical aortic valve. From these 10 patients, a consultation with cardiologist was made in five of them before starting LDOM treatment.
Systemic AE were reported in only one patient. This was a patient with supraventricular extrasystole who was treated with carvedilol. This patient developed periorbital and pedal edema with LDOM 1 mg and the swelling resolved after adjusting the dose to 0.25 mg. No patients reported palpitations, worsening of their prior arrhythmia or any other cardiac side effects, and none of them required a modification of their prior medical treatment.

Summary
This is an interesting study as it represents the first study of the safety of LDOM in patients with HT or arrhythmia.
It’s important to have this data. The global prevalence of HT in adults is 34%,so there are going to be numerous patients that come to us looking for treatment options who happen to have high blood pressure.
The authors found that for the most part side effects were fairly similar to the array of side effects seen in patients without hypertension and arrythmia. However, there were 2 side effects that were more common in those with hypertension and arrhythmia treated with LDOM – fluid retention and light headedness.
Many patients with light headedness and tachycardia in this study needed to reduce their dose or stop. Patients with hypotrichosis generally just needed to reduce their dose rather than stop.
Lightheadedness was seen in 7% and the most common reason for patients to need both adjustment and discontinuation of LDOM
Key Recommendations by Authors
What I really liked about this paper is that the authors conclude by offering some helpful recommendations and cautions. They propose that most patients with hypertension can start LDOM without referral to a cardiologist. Starting the dose at bedtime may limit the chances of postural hypotension
The authors propose that Caution is warranted in those using 3 or more drugs, those using the drug doxazocin and those with uncontrolled hypertension or arrythmia . These patients may benefit from cardiologist referral as well as baseline EKG and proper monitoring of pressure measurements at home in the first few days and weeks of starting (and any dose adjustment)
The authors propose that some patients should not start LDOM at all including those with prior heart attacks, heart failure (especially with reduced ejection fraction), valvular disease, pericardial disease and kidney disease. These patients are probably not candidates at all but consultation with a cardiologist is necessarily.

REFERENCE
Jimenez-Cauhe J et al. Safety of Low-Dose Oral Minoxidil in Patients With Hypertension and Arrhythmia: A Multicenter Study of 264 Patients. Actas Dermosifiliogr. 2023 Aug 29:S0001-7310(23)00679-8.
This article was written by Dr. Jeff Donovan, a Canadian and US board certified dermatologist specializing exclusively in hair loss.