Oral Minoxidil Helps Traction Alopecia in Female Patients
Mild Improvements Noted with Oral Minoxidil Use in 57 Female Patients with Traction Alopecia
Oral minoxidil has shown to be helpful for the management of traction alopecia. Prior authors, including Beach in 2018 and Kim and Craiglow in 2022 showed good outcomes for oral minoxidil. Beach described 4 patients with TA who were treated with oral minoxidil 1.25 mg nightly. 3 were able to use the medication with benefits although 1 stopped due to pill aversion.
Kim and Craiglow described a nice case of regrowth from use of oral minoxidil. The patient was a 31 year old female with traction alopecia. She had a history of wearing tight hairstyles in the past and was presently using chemical relaxers. She had been treated with topical steroids and minoxidil in the past without improvement. The patient was then started on oral minoxidil 1.25 mg daily and also used fluocinonide 0.05% topical solution 2-3 times weekly for the first 2 months. After 6 months of using the oral minoxidil, there was notable regrowth of hair, and minoxidil was increased to 1.25 mg twice daily (2.5 mg total dose). After an additional five months of the treatment (11 month total), there was continued regrowth of hair on the bilateral frontotemporal scalp. The patient continued to use chemical relaxers throughout this time.
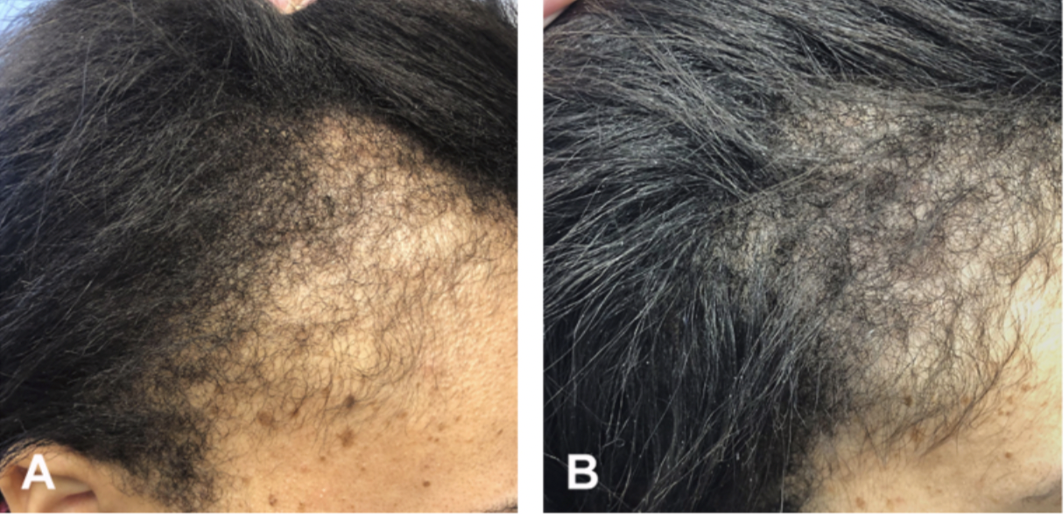
Improvement in traction alopecia with 2.5 mg oral minoxidil. SOURCE: Kim and Craiglow. Treatment of traction alopecia with oral minoxidil. JAAD Case Rep. 2022 Apr 1;23:112-113. used with creative commons license
Awad et al 2023
In a new study, Awad and colleagues set out to retrospectively reviewed the records of patients with TA age over 12 years who had been treated with low dose oral minoxidil LDOM for 6 months or more. The severity of hair loss before and after treatment was determined using the marginal TA severity (M-TAS) score. This scoring system combines the scores of the anterior (0-9) and posterior (0-9) margins to a maximum score of 18.
58 patients were included in the study. Mean onset of TA was 32.7 years. The mean duration of hair loss was 6.4 years. Most patients in this study were female although one was male. 75.9% were White and 10.3 % were Black, 8.6 % were Middle Eastern, 3.4 % were South Asian and 1.7% were East and Southeast Asian
The cause of the traction alopecia was tight ponytails in 37.9%, tight buns in 12.1 %, hair extensions in 12.1%, braids in 8.6 %, hair clips in 6.9% and dreadlocks in 3.4 %
The mean starting dose was 0.75 mg and the dose was titrated upwards if there was suboptimal growth and the mean final dose was 2.5 mg.
What were the results?
All in all, treatment with LDOM helped hair growth and the mean M-TAS score decreased from 5.1 to 3.6
Side effects included hypertrichosis in 22.% and light headedness in 5.2 % and none of the patients need to reduce or stop treatment.
Comments
This is another helpful study that highlights the benefits of oral minoxidil for treating traction alopecia. This study was mainly a study of traction alopecia in white women although 10 % were black. This was also a study of TA in longstanding disease with the mean duration being 6.4 years.
The results showed a mild improvement - rather than profound improvement. The results here remind us that long standing traction alopecia is still not easy to treat.
We don’t have a sense of patient satisfaction and what proportion of the 58 patients felt this was a good outcome. That would be helpful to know.
The mean final dose was 2.5 mg which is high! that means that many women were on more than this dose. I only prescribe 2.5 mg to 15-20% of females in my practice as I find many don’t tolerate these high doses all that well but do tolerate 1.25 and 1.875 mg fairly well. I was surprised at the high doses.
Finally, a key questions here is “what happens when oral minoxidil is stopped?” I don’t think we really understand what happens when oral minoxidil is stopped. The authors stated that “it is likely that improvements would be maintained upon cessation of therapy providing tight hairstyles were avoided.” I think this is a big leap in interpretation. First, we can’t be sure there is no some degree of minoxidil dependence here. Second, we expect 10% to 15 % of women to have some degree of androgenetic alopecia, even if it is subclinical. The cessation of oral minoxidil may serve to trigger a telogen effluvium and potentially worsen underlying androgenetic alopecia. In my view, the cessation of oral minoxidil is a big deal but more studies are needed.
REFERENCES
Awad A et al. Low-dose oral minoxidil improves hair density in traction alopecia. J Am Acad Dermatol. 2023 Feb 24;S0190-9622(23)00278-5.
Beach RA. Case series of oral minoxidil for androgenetic and traction alopecia: Tolerability & the five C's of oral therapy. Dermatol Ther. 2018 Nov;31(6):e12707.
Kim and Craiglow. Treatment of traction alopecia with oral minoxidil. JAAD Case Rep. 2022 Apr 1;23:112-113.
This article was written by Dr. Jeff Donovan, a Canadian and US board certified dermatologist specializing exclusively in hair loss.