Incidence and Prevalence of LPP are Rising in Korea
Six fold Rise in LPP Incidence over 2003-2019 Period of Study
A new study from Korea set out to investigate the prevalence, incidence, and clinical characteristics of LPP in Korea. To do so, the authors used data from the National Health Insurance Service database of Korea (NHIS). The NHIS is operated by the Korean government and includes approximately 99% of the Korean population.
Only patients who had ≥3 documented visits with an International Statistical Classification of Disease, 10th revision (ICD-10) code of L66.1 (lichen planopilaris) from 2003 to 2019 were considered as LPP patients. Presumably, LPP and FFA were grouped together in this study. To include only incident cases, LPP patients with medical visits dated before 2003 were excluded. The incidence and prevalence of LPP were calculated during the 2003-2019 study period. In terms of controls, age, sex, insurance type, and income level-matched individuals without documented visits of LPP during the whole observational period were selected, to compare the comorbid conditions
RESULTS
A total of 2992 patients with LPP and 59 840 matched controls were identified. There was slight female predominance (male-to-female ratio, 1:1.24), and age with peaks in the 40–50s and teenage years. The incidence rose from around 1 per 1,000,000 in 2006 to 6 per 1,000,000 in 2019. Annual prevalence rose from around 2 per 1,000,0000 in 2006 to 11.38 per 1,000,000 in 2019. In other words, there appears to be a six fold increase in incidence or annual prevalence during this time. According to cumulative incidence data, there are now at least 5 people with LPP per 100,000 population in Korea (1 in 20,000).
Overall, data indicated that LPP incidence and annual prevalence have increased over the last 17 years. Peak incidence was observed during the summer. The incidence was 36 % higher in urban than in rural areas,
CORMORBIDITIES
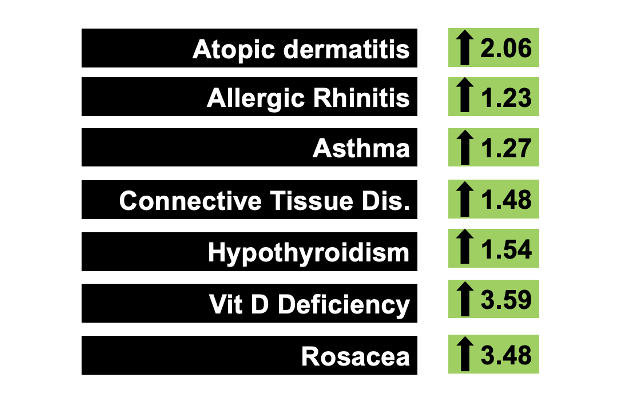
The more prevalent comorbid conditions in patients at LPP diagnosis compared to controls were atopic dermatitis (odds ratio [OR], 2.06; 95% confidence interval [CI], 1.89–2.24), allergic rhinitis (OR, 1.23; 95% CI, 1.15–1.33), and asthma (OR, 1.27; 95% CI, 1.17–1.38), autoimmune connective tissue diseases (such as RA, SLE, Scleroderma, ankylosing spondylitis); OR, 1.48; 95% CI, 1.17–1.87), hypothyroidism (OR, 1.54; 95% CI, 1.30–1.83), vitamin D deficiency (OR, 3.59; 95% CI, 2.34–5.51), and rosacea (OR, 3.48; 95% CI, 1.20–10.07). These are summarized in the figure below.
Comments and Discussion
This is an interesting study. We don’t know if theses patients had LPP as these are simply codes entered in a computer as opposed to truly verified cases. Further, it’s not clear if these cases were mostly LPP or a mix or LPP and FFA. Presumably it’s a mix and the same ICD code was used for LPP as for FFA.
Overall, it appears that the diagnosis of LPP has increased dramatically over the 17 years of the study. It was interesting that so many teenage patients are receiving diagnoses of LPP.
The seasonal change in LPP is interesting but it’s not clear if there are truly confounders here or not. There was a peak in the summer and then again in November with a smaller speak. One would assume these are the dates when diagnoses are entered into the computer apparently rather than actual diagnosis. If a person develops LPP in Sept 2021 and is seen in the clinic in July 2022 are they considered to have LPP in Sept 2021 or July 2022? It would appear in this study that it would be July 2022. Data of this kind is challenging to interpret and the authors did not clarify for us.
An increased incidence of LPP in urban areas vs rural areas was identified. Whether this is related to pollution, different lifestyles (such as excessive hygiene), or confounders is not really clear.
I really liked this study as it documents a very significant rise in cases. It may be that LPP is less common in Korea than the USA. Prior studies in New York put incidence at around 13 per 100, 000 (1 in 7700) for combined LPP and FFA. It would appear that LPP in Korea may be less than what is seen in New York but of course more studies are needed.
REFERENCE
Ha Lim S et al. Rapidly increasing incidence and prevalence of lichen planopilaris in an Asian population: A Korean nationwide population-based study. J Dermatol. 2022 Jun 21.
Lavian J et al. Incidence estimates for lichen planopilaris and frontal fibrosing alopecia in a New York City health care system. Dermatol Online J. 2021 Aug 15;27(8).
This article was written by Dr. Jeff Donovan, a Canadian and US board certified dermatologist specializing exclusively in hair loss.