5 Common Mistakes in Prescribing Oral Minoxidil for Women's Hair Loss
Prescribing Oral Minoxidil for Hair Loss in Women: 5 Common Mistakes
When it comes to treating hair loss, what’s “new” is generally also what’s popular too. I’m not saying it should be this way - just it usually is. This is certainly true for oral minoxidil. It is increasing prescribed by physicians for treating hair loss. Oral minoxidil was used in the 1970s and 1980s at doses ranging from 20-60 mg (and sometimes even higher too) for treating high blood pressure. 80 % to 90 % of patients using oral minoxidil for treating their blood pressure problems grew hair on the head and body - and this lead to the exploration and ultimately development of a topical form of minoxidil. 10-15 years ago oral minoxidil found a resurgence in clinical medicine - this time for treating hair loss. Instead of using doses like 20-60 mg, hair clinicians turned to using small doses 0.25 mg to 5 mg. interestingly, these doses helped treat hair loss and were associated with dramatically fewer side effects than the much higher ‘blood pressure’ doses.
Oral minoxidil is increasingly used nowadays. it’s not FDA approved for treating hair loss so its use for hair problems is said to be entirely ‘off label.’ The treatment is helpful for many patients - but also a treatment coupled with troublesome side effects when a few key rules are ignored.
Here, I review 5 common mistakes that I see clinicians and patients make when prescribing and using oral minoxidil for women with androgenetic hair loss.
ERROR 1: Patients are started on too high of a dose of oral minoxidil.
There’s no doubt in my mind that many patients simply start out with too high of doses of oral minoxidil. There are no rules per se since the treatment is entirely off label. But I see too many women started at a does of 2.5 mg.
Most women tolerate 0.25 mg to 1.25 mg without difficulty. In fact, most tolerate 1.25 mg without problem. But not all do! Once one goes beyond 1.25 mg, that’s when we start to increase our chances of side effects.
Data from a very nice study in 2020 by Ramos and colleagues gave us some really valuable information about what side effects we might expect when female patients use 1 mg of oral minoxidil to treat female pattern hair loss. What are the statistics? 4 % of users of oral minoxidil at 1 mg develop swelling in the feet, a 27% develop excessive hair and many experience a slight increase in heart rate (an average of 6 beats per minute). As we will see in just a moment when we talk about the Sanabria et al study , about 10 % of women on 1.25 mg and less get headaches, 9 % get swelling in the feet and 54 % experience excessive hair growth.
Simply put, doses beyond 1.25 mg can lead to a great proportion of patients having side effects. That’s when we start to see fluid retention and dizziness and heart rhythm issues. Is the risk still pretty low with doses just slightly exceeding 1.25 mg ? Sure. But if you are a patient sitting at home on Saturday night with dizziness and can’t get a hold of the doctor, it’s absolutely terrifying.
80-85 % of my female patients are on doses 1.25 mg or less. 15 % or so are on the 1.875 mg and 2-3 % are on doses 1.875 mg to 2.5 mg. This dosing protocol for women is in contrast to the dose we use in men where 2.5 mg to 5 mg is a more typical dose.
I generally start 0.625 mg for 1-2 weeks and then go up to 1.25 mg. I stay on this dose for 4-6 months. If the patient is tolerating is really well (no headaches, no fluid retention, no excessive hair growth), I may discuss with the patient the option to go to 1.875 mg (3/4 of a 2.5 mg pill) or alternate 1/2 pill with 3/4 pill. If the patient is very pleased with the hair regrowth at the 6 month mark one 1.25 mg, we may not go up any more. Many patients stay on 1.25 mg.
ERROR 2: Patients increase the dose of oral minoxidil too quickly.
There are no rules per se in how oral minoxidil is to be dosed. For those who are young and healthy and have normal baseline blood pressure (115-125 systolic), I often start 1/4 of a 2.5 mg pill (ie 0.625 mg) for 1-2 weeks and then go right up to 1/2 pill. For some, I go a bit slower.
It’s common, in my opinion, to increase the dose too fast.
In order to understand why being cautious makes the most sense, it’s important to understand when exactly side effects are expected to occur. Do side effects happen in hours if they are going to happen? … or does it take days or weeks? Well, the various side effects of oral minoxidil happen at different times.
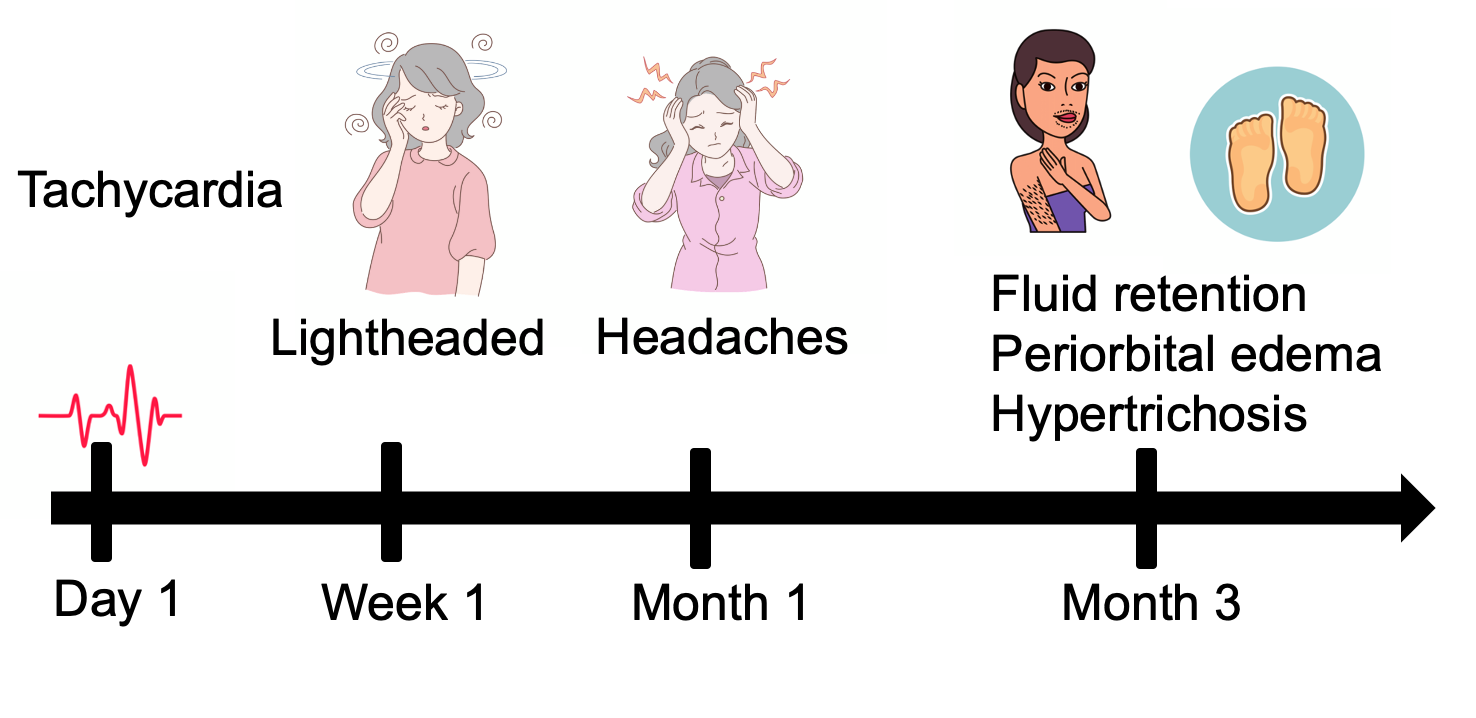
Heart rate problems happen within hours to days if they are going to occur at all. Light headedness occurs within the 5-10 days if it’s going to occur and dizziness occurs sometime within the first month. Now for the key statistic - fluid retention and hair growth on the body does not start to become apparent until around month 3 after starting.
To reiterate, I often start 1/4 of a 2.5 mg pill (ie 0.625 mg) for 1-2 weeks and then go right up to 1/2 pill. For some, I go a bit slower. I then patiently wait and wait and wait to see what the body thinks about this dose. Fluid retention takes many months to show up so I don’t go up on the dose simply because everything seems fine. I wait for a few months at the 1/2 pill dose. if fluid retention does not occur and hair growth on the face of body issues not excessive , I might go up on the dose if the patient is not pleased with the results. Usually I wait a full 6-7 months to decide on this.
ERROR 3 - We underestimate the chances of side effects from oral minoxidil.
I truly think that we all want oral minoxidil to work for our patients. The excitement of oral minoxidil is what PRP was a decade ago. Many patients wants to try it. Many clinicians want to prescribe it.
In my opinion, I think we need to respect the side effects of oral minoxidil. I’m as much of an expert in oral minoxidil side effects as I am an expert in the actual use of the drug to treat hair loss. If you think oral minoxidil does not have all sorts of side effects, it just means you have not prescribed it enough. Plain and simple.
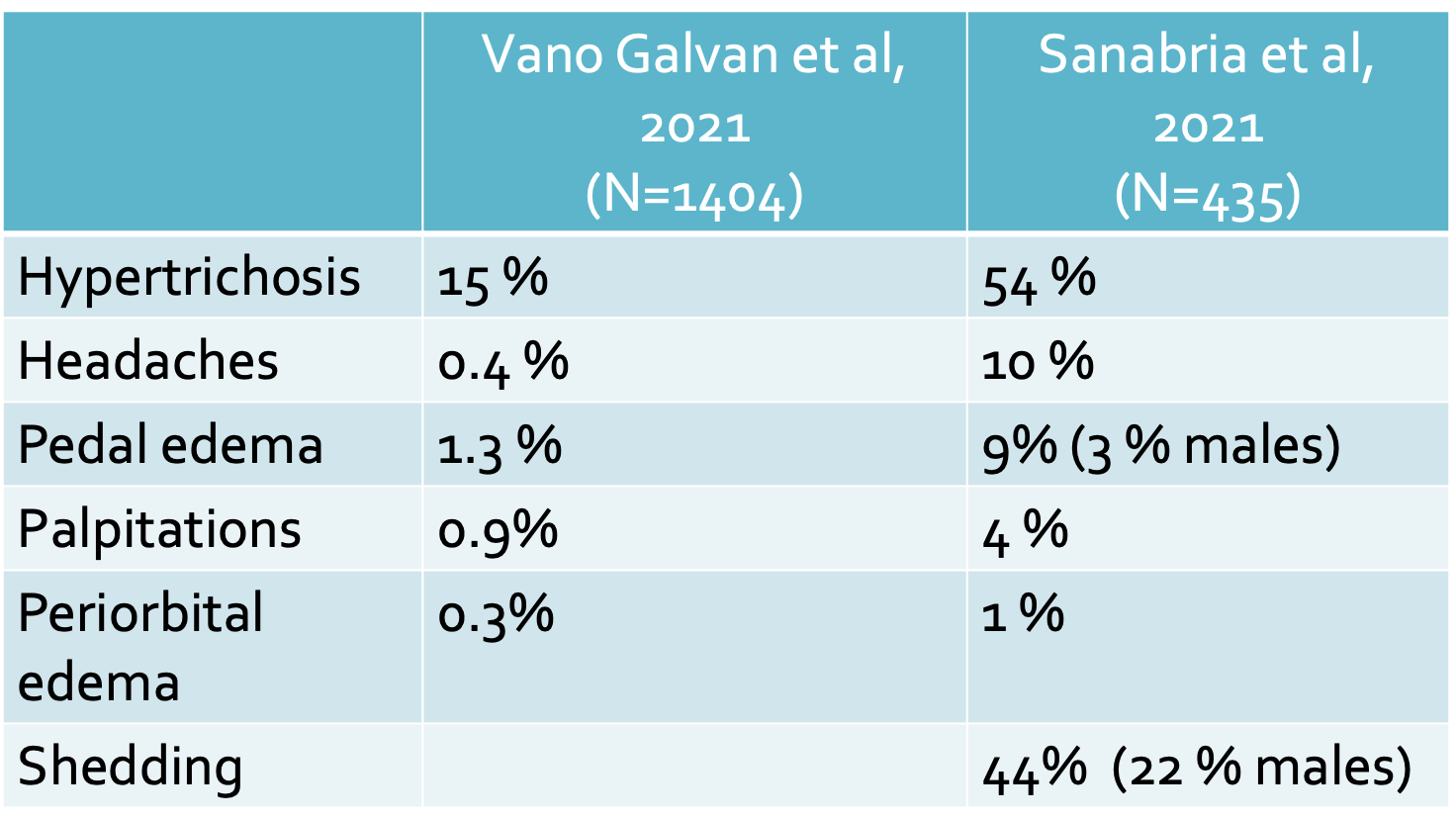
We don’t really know the true incidence of all the side effects. Not at all. We only have estimates from different types of studies - all which have their inherent flaws in collecting data. Two very nice studies give us some useful data on the frequently of side effects with oral minoxidil. These are studies by Vano-Galvan et al and Sanabria et al. Clinicians who prescribe oral minoxidil in their practices really need to dig out these two studies and read them. Hypertrichosis (excessive hair) occurs in 25-50 % of patients treating with oral minoxidil. The proportion of patients with hypertrichosis was higher in the Sanabria et al study than the Vano Galvan et al study, but the Sanabria et al study involved directly asking patients whereas the Vano-Galvan study involved directly asking the treating doctors. Headaches, pedal edema (feet swelling) and heart palpitations are all every much part of the array of side effects and why patients might contact their doctors after being prescribed this drug. You can review the proportion of patients who are likely to be affected by these issues in the charts below. Shedding is another side effect of oral minoxidil that is somewhat poorly described in the medical literature. Sanabria et al suggested that nearly 44 % of women using fairly standard minoxidil doses (0.625 mg to 1.25 mg) get shedding.
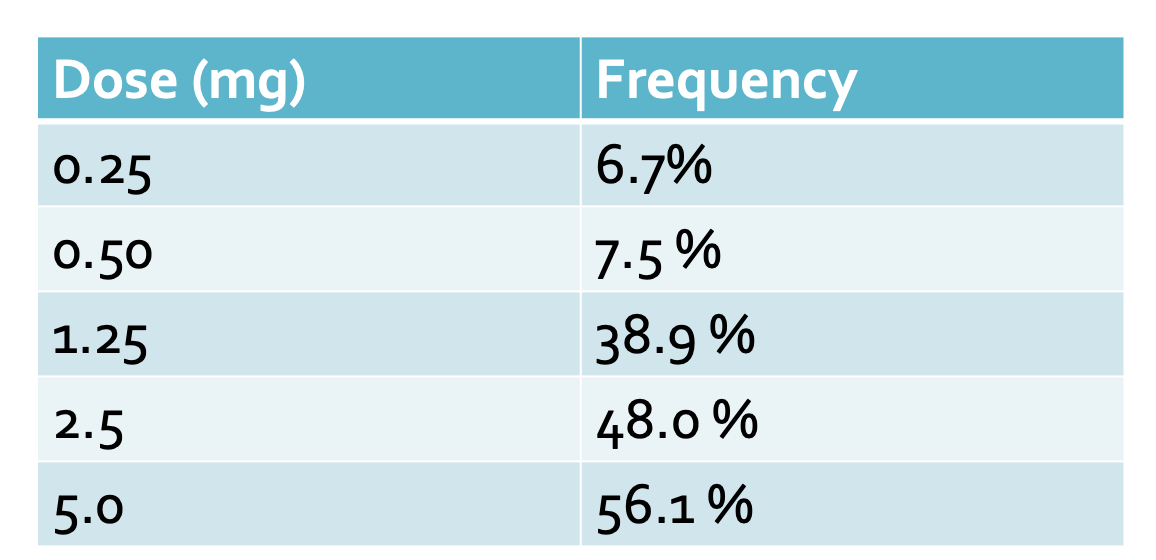
Hypertrichosis (excessive hair on the body) is very much a dose-dependent side effect of minoxidil. Studies by Jiminez-Cauhe and colleaguees shows that the chances of hypertrichosis increase dramatically with higher doses.
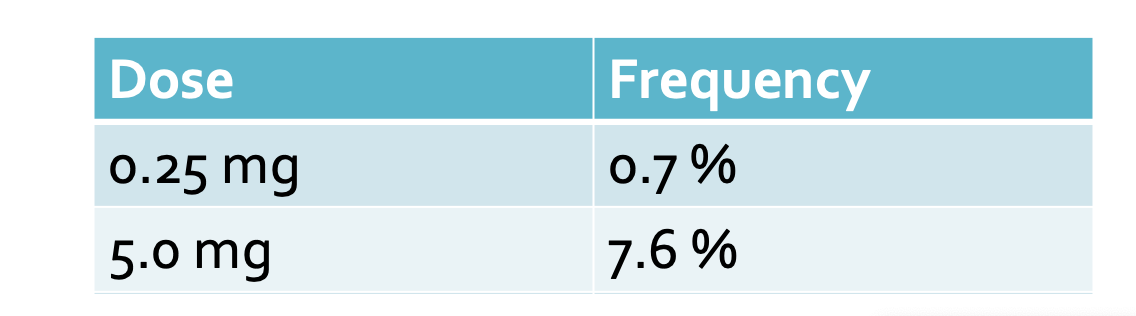
The same is true of pedal edema (swelling in the feet). Studies by Jiminez-Cauhe and colleagues showed that the chances of pedal edema increase dramatically with higher doses.
ERROR 4: We stop the oral minoxidil too soon without a sufficiently long trial to see if it actually helps.
Oral minoxidil is a treatment that more or less respects the basic rules of hair growth. It takes 4-6 months to show results and even a bit longer to really show maximal results (if they actually are going to occur).
I see patients every week who tell me they used oral minoxidil for a few weeks or a few months and that it had no effect. In my mind, these patients have not used oral minoxidil at all. it takes 4-6 months to see whether or not minoxidil works or not and ideally I like to give patients 6-7 months of a trial.
ERROR 5: We decrease the dose of oral minoxidil when we should not be adjusting the dose.
Finally, I am increasingly encountering patients who tell me that the use of high doses of oral minoxidil is a temporary treatment and that once nice growth starts happening they can reduce the dose a bit. The story usually goes something like this. Patients can start oral minoxidil once daily and then once they get good growth they go down to three times per week.
Nothing is further from reality.
Anyone who starts oral minoxidil for treating androgenetic hair loss should plan to use it lifelong at the dose they were prescribed. If they choose to increase the dose beyond what they were prescribed, they increase their chances of side effects a little bit (as well as the chances it might help more). However, it the patient chooses to decrease the dose below what they were prescribed, they run the risk of losing hair.
What does the hair say when a patient using 1.25 mg of minoxidil daily decides to go down to using it Monday to Friday only? The hair does not like it and the patient experiences hair shedding !
What does the hair say when a patient using 1.25 mg of minoxidil daily decides to stop using it on vacations and trips away and on weekends? The hair does not like it and the patient experiences hair shedding !
CONCLUSION
Oral minoxidil is proving to have a place in the treatment of hair loss in women. The drug, however, has possible side effects that need to be carefully discussed with patients. Some of the side effects like heart palpitations and dizziness are not common but if they are going to occur they occur soon after starting the drug. Other side effects like fluid retention and hair growth on the body take months and months to develop. For this reason, one needs to be patient to observe the benefits and side effects of the drug before deciding on whether or not to increase the dose.
Finally, it needs to be mentioned that many rush to using oral minoxidil because of how new this treatment is and the feeling that anything new is better. Anyone using oral minoxidil needs to have first given very careful through to whether “topical minoxidil” is actually a better option for them. For many women, oral minoxidil at 1.25 mg is fairly equivalent in effectiveness to 5 % minoxidil. Not everyone, but many. That’s a sixth error in minoxidil prescribing - but a topic for another article.
REFERENCES
Jimenez-Cauhe et al. Safety of low-dose oral minoxidil treatment for hair loss. A systematic review and pooled-analysis of individual patient data. Dermatologic Therapy 2020. 33:6
Ramos et al. Minoxidil 1 mg oral versus minoxidil 5% topical solution for the treatment of female-pattern hair loss: A randomized clinical trial. JAAD 2020; 82(1): 252-253.
Sanabria B et al. Adverse effects of low dose oral minoxidil for androgenetic alopecia in 435 patients. JAAD 2021; 84: 1175-78
Vano-Galvan S et al. Safety of low dose oral minoxidil for hair loss: A multicenter study of 1404 patients. JAAD 2021; 84: 1644-51.
This article was written by Dr. Jeff Donovan, a Canadian and US board certified dermatologist specializing exclusively in hair loss.