The Diagnosis of Polycystic Ovarian Syndrome in Teenagers/Adolescents
How is PCOS Diagnosed in Teenagers?
About 10 % of women have a diagnosis of polycystic ovarian syndrome, making it one of the most common endocrine disorders of premenopausal women. About 70 % of women with PCOS are thought to be undiagnosed. About 6 % of adolescent females have PCOS so this is an important diagnosis to know about.
Before we examine how PCOS is diagnosed in adolescents, let’s review the diagnosis of PCOS in adults as that we help us better understand the logic of the criteria for diagnosing PCOS in adolescent females. Most women with PCOS have irregular periods and evidence of clinical or lab evidence of increased androgens (which we call ‘hyperandrogenism.)’. Hair growth on the face (hirsutism), or abdomen, chest, nipples, along with hair loss and acne are common “clinical” signs of hyperandrogenism in women with PCOS. Other symptoms include heavy periods, headaches, darkening of the skin (acanthuses nigricans), skin tags, diabetes, pre-diabetes, high blood pressure, high cholesterol obesity, and infertility. Women with PCOS are at increased risk for cardiovascular disease and uterine cancer.
I have discussed the diagnosis of PCOS in adults in several prior articles. Genetic, hormonal (high androgens), inflammatory and endocrine (insulin resistance) issues contribute all contribute to this complex disease. The diagnosis of PCOS does not actually require every patient suspected of having this diagnosis to have an ultrasound in order to make the diagnosis. Both the Rotterdam Criteria and the Androgen Excess PCOS Criteria have polycystic ovaries on ultrasound as one of the “criteria” that can be used in making the diagnosis - but it’s not a mandatory criterion. If the patient fulfills the criteria for PCOS diagnosis with use of the other 2 criteria, then ultrasound is not really needed. Of course, many women who are being evaluated for PCOS have full evaluations, blood tests and ultrasounds.
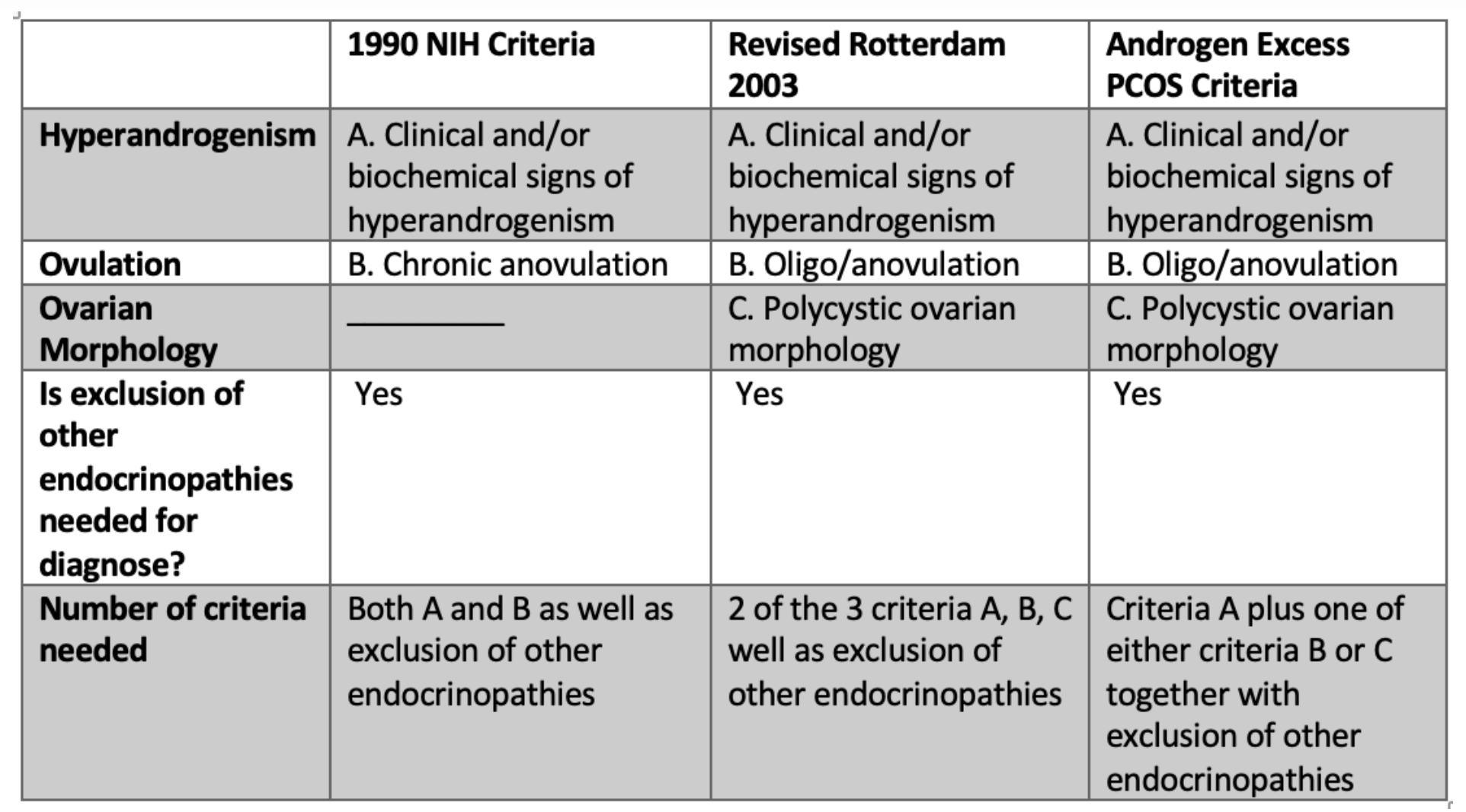
ADULTS: Criteria for Diagnosis of PCOS in Adults
The adult criteria for diagnosis for PCOS are shown below. Both the 2003 Rotterdam Criteria and the 2008 Androgen Excess criteria are frequently used and both are similar in many regards. “Irregular periods” are a feature of both the Rotterdam criteria and the Androgen Excess criteria and may involve anovulatory cycles in which an egg is not released mid cycle or cycles that are greater than 35 days (or less than 21 days). Anovulatory cycles can be measured by performing a day 21 progesterone blood tests and showing that level of progesterone do not rise as expected. It must always be remembered that even women with apparently regular menstrual cycles can be having anovulatory cycles. Hyperandrogenism is defined either by finding that androgens blood tests are elevated or the patient has signs of hyperandrogenism on the skin like acne or hirsutism. As far as blood tests, free testosterone or total testosterone are the key tests (or relying on DHEAS or androstenedione if all testosterone tests are normal). Free testosterone is probably the best but it’s difficult to find labs that measure precisely. It should be noted that these blood tests must be done with women off oral contraceptives for at least 3 months.
The diagnosis of PCOS in adults requires exclusion of other endocrine disorder such as thyroid disorders, pregnancy, prolactin related issues, Cushing’s disease, late onset congenital adrenal hyperplasia, androgen secreting tumours, hypothalamic amenorrhea, primary ovarian insufficiency and acromegaly.
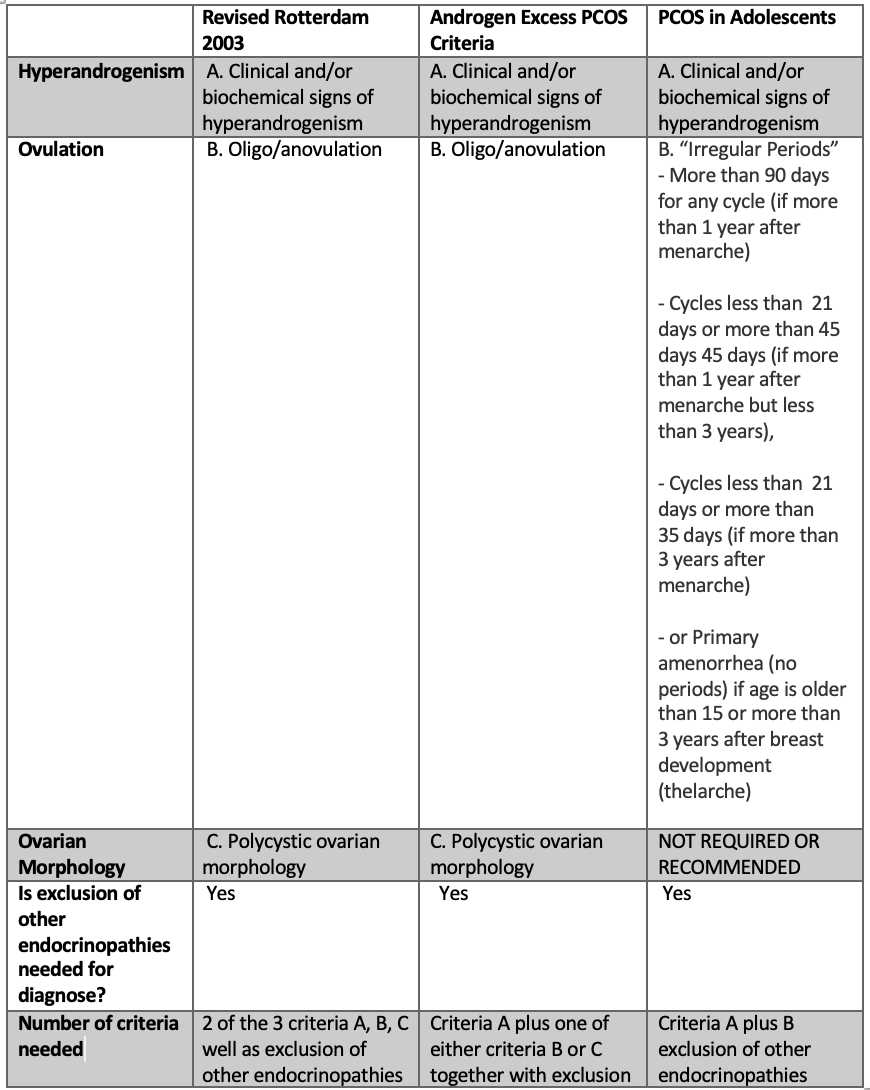
ADOLESCENTS: Criteria for Diagnosis of PCOS in Adolescents
As we begin now to discuss the diagnosis of PCOS in adolescents, we need to first understand what might be considered a ‘normal’ period in adolescent females. First, it’s important to remember that menstural cycles are normally quite irregular to some degree in the first few years after menarche (the age of the first menstruation). In the first year, cycles are often very irregular. Again, that’s completely normal. Because of this, the diagnosis of PCOS in adolescents its not possible unless more than 1 year has passed since the onset of menstrual cycles. In the first three years after menarche, normal cycles can range from 21 to 45 days. If cycles are less than 21 days or more than 45 days, then that’s considered abnormal. if more than three years has passed since menarche, a normal cycle is considered 21 to 35 days. It’s rare for adolescents to be having periods longer than 35 days beyond the first 3 years.
The diagnosis of PCOS in adolescents is different than in adults because we don't require (or even recommend) the use of ultrasound examinations. Ultrasounds are NOT recommended in the first 8 years after menarche (the age at which menstrual cycles first start).
With the exception of ultrasounds, the diagnosis of PCOS in adolescents is somewhat similar to adults. Although ultrasounds are not needed, the diagnosis in adolescents requires “irregular periods” and “hyperandrogenism.” The exact definition of irregular periods depends on the length of time that has transpired since menarche (the time of the first period) and the age of the patient. Again, it’s worth repeating again that a diagnosis of PCOS is not possible if it has been less than 1 year since that start of menarche because irregular menstrual cycles are normal during this time.
Summary of Criteria for Diagnosis of PCOS in Adolescents
(1) Irregular menstrual cycles or lack of menstrual cycles (see definitions above)
(2) Hyperandrogenism, defined as
· Hirsutism or severe acne or andoagenetic alopecia
· and/or biochemical hyperandrogenaemia confirmed using validated high-quality assays.
(3) Exclusion of other endocrine disorders that mimic PCOS including congenital adrenal hyperplasia, Cushing syndrome, prolactinomas, androgen secreting tumours, thyroid disease, hypothalamic amenorrhea, primary ovarian insufficiency and acromegaly.
Adolescents are said to be “at risk” if they have features of PCOS but do not meet diagnostic criteria above. These individuals require frequent re-evaluation.
Comment on Use of Ultrasound in Adolescents
I’m often asked in adolescents with suspected PCOS should have ultrasound examinations. The answer for most adolescents is quite straightforward: No! Ultrasounds are not helpful because polycystic ovarian morphology is so common normally in adolescents and does not mean the individuals has PCOS. Ultrasound tests are only useful if it has been MORE THAN 8 years since menarche.
But even if an individual is now more than 8 years since her first period and PCOS is a possible diagnosis that is being considered, an ultrasound is NOT necessary for the diagnosis of PCOSS if she has irregular periods and high androgens on blood tests. The diagnosis of PCOS has been confirmed without the need for ultrasound!
If it is decided that ultrasound is going to be done for further evaluation of PCOS, one really needs the patient to go to an experienced radiology clinic that scans a lot of women. It takes an experienced ultraound technician to generated a good and consistently helpful report. That’s another story but one must not forget this point. Second, one needs to decide if “transabdominal” or “transvaginal” ultrasound testing is going to be done. In a transabdominal scan, the ultrasound probe is placed on the abdomen. In a transvaginal scan, the probe is placed in the vagina.
Transvaginal ultrasound is best as it allows follicle number to be properly assessed - provided that modern ultrasound transducers are used to scan the patient. An accurate assessment of follicle number can not be done with transabdominal ultrasound. The same principle is true for both adolescents and adults. A transvaginal ultrasound is generally considered only if the patient is sexually active and the test is considered acceptable to the patient.
If transabdominal ultrasound is done, a “positive test result” would be the measurement of either ovary as more than 10 mL. There is no role for assessing follicle number with the transabdominal scan as the scan is not sensitive enough to assess this. If transvaginal ultrasound is done, a “positive test result” would be measurement of either ovary as more than 10 mL or the finding of more than 20 follicles per ovary. (The prior cut off was much lower so readers should note the new number of 20).
Final Summary
The diagnosis of PCOS in adolescents requires some evidence of “irregular periods” and some evidence of “hyperandrogenism.” Ultrasound scans are not to be done if it has been less than 8 years since the time of the first period. A proper history and physical examination along with blood tests are necessary to rule out other medical conditions.

REFERENCES OF INTEREST
Ibáñez L et al. An International Consortium Update: Pathophysiology, Diagnosis, and Treatment of Polycystic Ovarian Syndrome in Adolescence. Horm Res Paediatr. 2017;88(6):371-395. doi: 10.1159/000479371. Epub 2017 Nov 13. .
This article was written by Dr. Jeff Donovan, a Canadian and US board certified dermatologist specializing exclusively in hair loss.