Minoxidil and Spironolactone: Are they causes of tinnitus?
Tinnitus in the Patient Using Minoxidil and/or Spironolactone: Is it related or just a coincidence?
Tinnitus, commonly called “ringing in the ears”, refers to sounds that patients hear despite the fact that those sounds are not present. Tinnitus is very common in the population. This means that many patients in the hair loss clinic will report tinnitus.
What is tinnitus?
Tinnitus refers to the perception of sound in one ear or both ears in the absence of an external source that would be responsible for generating that sound. Although tinnitus is commonly called ‘ringing in the ears” the sound may be more than just ringing - buzzing, hissing, sizzling and whooshing are commonly described too. About 50 % of people experience this in both ears and 50 % have tinnitus in just one side (the left is favoured for reasons that are unclear).
How common is tinnitus?
Tinnitus is common. About 15 % of the adult population has experienced tinnitus. Studies across various countries including Egypt, Japan, Nigeria and the US suggest rates are similar. One study estimated that about 50 million people in the US have experienced tinnitus and about 16 million experience it frequently.
What are the common causes?
There are many causes of tinnitus. When the exact cause can not be found, a person’s tinnitus may be referred to as ‘primary’ or ‘idiopathic’ tinnitus. When an underlying cause for the tinnitus is found, the tinnitus is referred to as ‘secondary’ tinnitus.
Tinnitus can be associated with the following conditions and risk factors:
1. Hearing loss. The main risk factor for tinnitus is hearing loss. For this reason, it is essential that everyone with tinnitus have a hearing test.
2. Acoustic neuromas (schwannomas).
3. Ear diseases. Various inner ear, middle ear and outer ear diseases can cause tinnitus.
4. Depression and Anxiety. A link between these conditions and tinnitus has been demonstrated in several studies.
5. Drugs. The most common drugs causing tinnitus are aspirin and NSAIDs, benzodiazepines, tricyclic antidepressants, antibiotics (gentamicin) and isotretinoin. Blood pressure pills including loop diuretics, ACE inhibitors, angiotensin receptor blockers, thiazide diuretics, potassium-sparing diuretics, and calcium channels blockers are rare causes. The antimalarial drugs chloroquine and hydroxychloroquine can also give tinnitus.
6. Vascular issues. Disease of the blood vessels are sometimes associated with a ‘pulsatile’ tinnitus
7. Hypertension
8. Immune diseases - rheumatoid arthritis, lupus, multiple sclerosis
9. Endocrine issues- hypothyroidism
10 TMJ disease - diseases of the temporomandibular joint
11. Caffeine intake.
A Word on Tinnitus in Spironolactone and Minoxidil Users.
First, we’ll address the relationship between tinnitus and minoxidil first. Although some blood pressure medications have been associated with tinnitus on rare occasions, this is not something that is typically reported with the hair growth drug minoxidil. Minoxidil is not a likely culprit for the vast majority of people with tinnitus and other reasons should be activity sought to explain the tinnitus. In the 2011 review by Dr Cianfrone and colleagues called “Pharmacological drugs inducing ototoxicity, vestibular symptoms and tinnitus: a reasoned and updated” minoxidil is not even listed.
Now, let’s review what is known about spironolactone. In most people with tinnitus who use spironolactone, spironolactone will not found be the cause of their tinnitus. In the 2011 review by Dr Cianfrone and colleagues called “Pharmacological drugs inducing ototoxicity, vestibular symptoms and tinnitus: a reasoned and updated” the authors gave spironolactone a ‘category 3” rating. A category 3 rating is give to drugs that are “potentially vertigo-generating drugs, generally called vertigo or dizziness (drugs openly declared as vertigo generating). Information of potential vertigo associated with the drug is reported while there is no mention of ototoxicity.
Category 1 drugs are ototoxic. Category 2 drugs are known tinnitus inducers. Category 3 drugs like spironolactone are not known to be tinnitus inducers but do cause vertigo. Blood pressure medications like loop diuretics (Lasix) are category 1. ACE inhibitors are mostly category 3. Thiazide diuretics are category 3.
How does a patient know if it’s related to the drug?
As reviewed above, minoxidil is not likely the culprit of tinnitus for most people. Spironolactone is more common than minoxidil but is still very uncommon as a cause of tinnitus.
Tinnitus from drugs usually happens fairly quickly after starting the drug. The drug with the most rapid onset of tinnitus are the salicylates (ie aspirin). Following oral consumption or systemic injection of the drug, tinnitus presents within minutes and subsides within 72 h of the final dose. Blood pressure medications like furosemide also cause a fairly rapid onset of tinnitus.
For spironolactone users, tinnitus typically occurs in 2-4 weeks of startling the drug. Tinnitus occurring months after starting is not likely to be related to the drug.
Suggestions for Patients on Minoxidil and Spironolactone
For the vast majority of patients who use minoxidil and spironolactone, it’s important to note that the cause of tinnitus most likely has nothing to do with the use of minoxidil or spironolactone. If minoxidil or spironolactone was started within 2-4 weeks of the onset of tinnitus, it makes it a bit more likely there is a link. In these situations, I recommend stopping the drug for 1 week and seeing if the symptoms disappear and then restarting it again and seeing if the symptoms appear. A diary should be kept each day of the number of times the tinnitus occurred (or whether it was constant), the ear it was heard in and the type of tinnitus (pulsatile, etc).
Because these drugs are category 3 (non ototoxic), there is little harm in proceeding in this stop and start manner.
What investigations could a patient considering having if they have tinnitus?
1. Patients with tinnitus should first seek the attention of their primary care physician as this physician is best positioned to assess, investigate and provide appropriate counselling. The doctor will ask whether the tinnitus affects one ear or both, when it started and how it’s changing over time. The presence of tinnitus in one ear may raise concern to the doctor that a focal lesion could be present. The evaluatinng doctor will ask about other symptoms like dizziness, and hearing loss. Sudden onset of tinnitus associated with hearing loss requires prompt evaluation. It may require the patient to have an MRI imaging test and may require the patient to start a course of oral steroids,.
A full history will be taken by the primary care doctor during the evaluation of tinnitus. Blood pressure will be measured by the doctor. Ears will be examined. Bedside hearing and vibration tests (with a tuning fork) will be done. Basic neurological testing will be done. Blood tests may be ordered if deemed appropriate (ie thyroid studies, etc)
2. A formal audiology assessment (hearing test) is recommended for all patients who have tinnitus. Many patients with tinnitus have hearing loss so all patients with tinnitus should be evaluated with a hearing test.
3. Referral to an ENT (ear nose and throat) surgeon may be recommended if the cause of tinnitus is not clear or if further evaluation is needed.
4. Patients with tinnitus only on one ear (one side) or who have pulsatile tinnitus or who have asymmetric hearing loss or who have a focal neurological problem will likely be given a recommendation by their primary care physician to have further imaging tests done. This may include CT or MRI depending on the specific situation.
How is tinnitus treated?
If there is an underlying cause of the tinnitus (as there is in cases of ‘secondary tinnitus'‘), the goal of treatment is to address the cause. If a drug is thought to be causing the tinnitus, it is stopped. If a tumor is causing the tinnitus, it is treated. If depression and anxiety are contributing to the tinnitus, these are addressed.
There are no drug treatments for tinnitus that have proven effective.
In cases of primary tinnitus, hearing aids may be ordered for the patient if there is evidence of hearing loss. Sound therapy (provided by an audiologist) or cognitive behavioural therapies (provided by the primary care physician or a psychologist) are helpful therapies.
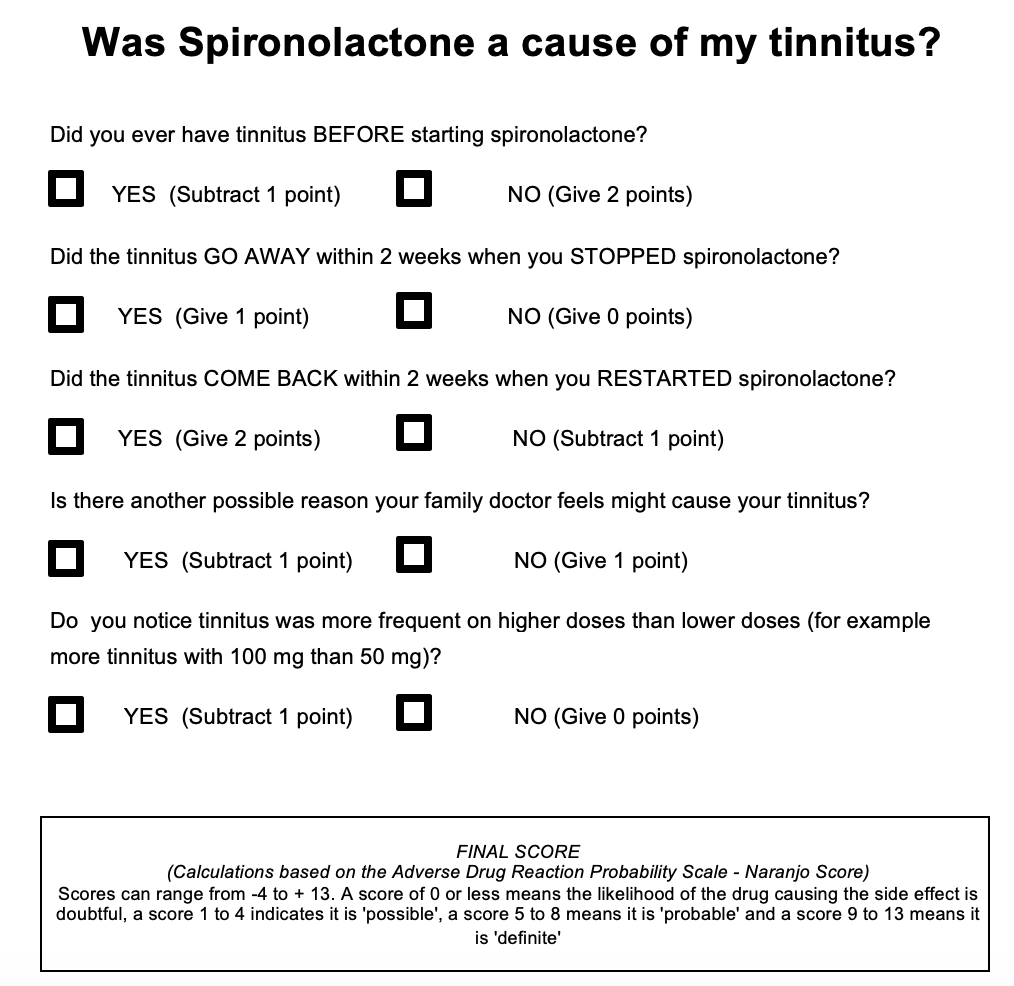
Patients of Dr. Donovan - please complete and submit to office
DOWNLOAD SPIRONOLACTONE TINNITUS RISK CALCULATOR
Reference
Baguley D et al, Tinnitus. Lancet. 2013; 382:1600-1607
Cianfrone et al. Pharmacological drugs inducing ototoxicity, vestibular symptoms and tinnitus: a reasoned and updated guide. Eur Rev Med Pharmacol Sci . 2011 Jun;15(6):601-36.
Khedr EM et al Epidemiological study of chronic tinnitus in Assiut, Egypt. Neuroepidemiology. 2010; 35: 45-52
Lasisi et al. Tinnitus in the elderly: profile, correlates, and impact in the Nigerian study of ageing.Otolaryngol Head Neck Surg. 2010; 143: 510-515
Michikawa et al. Prevalence and factors associated with tinnitus: a community-based study of Japanese elders.J Epidemiol. 2010; 20: 271-276
Mongan E. et al; Tinnitus as an indication of therapeutic serum salicylate levels. JAMA 1973; 226, 142–145.
Shargorodsky J et al. . Prevalence and characteristics of tinnitus among US adults. Am J Med. 2010 Aug; 123(8):711-8.
This article was written by Dr. Jeff Donovan, a Canadian and US board certified dermatologist specializing exclusively in hair loss.