Do I have AGA? Everything thinks I am Crazy!
Why am I losing hair ?
I’ve selected this question below for this week’s question of the week. It allows us to discuss the diagnosis of hair loss in the early stages and the use of the 5 day modified hair wash test.
QUESTION
Dear Doctor Donovan,
I'm a 27 year old female. I've seen a lot of dermatologists over the years but none of them could solve my problem and I'm desperate!! It's been three years that I'm losing hair. It started during a stressful period in 2018 with a significant amount of shedding (300-400 hair a day).
The shedding stopped for 4 months and then the shedding started again until now. The only thing I noticed during these years is that hair loss is focused on the side of the head and temples and hair always grows back, even if I have less. The dermatologists have all said the diagnosis is telogen effluvium or chronic telogen effluvium (CTE) because in their opinion I still have a lot of hair and no miniaturized hair (but I can see them!)
In 2019 I decided to starting using minoxidil 2% because I was losing my mind and I was scared to go bald. My mother uses it for AGA. I suffer from hypothyroidism, I have regular periods but low levels of ferritin. I'm also losing hair in different lengths (short, long, thick, thin).
I am afraid I have AGA. Nobody believes me and they think I'm crazy!.
Thank you very much for listening.




ANSWER
Thanks for submitting this very interesting question.
I’d like to discuss several important things in the question you ask and the information you have submitted.
Before we do go further, I’d like to point out that the ideal way to diagnose hair loss is using what I termed the ”Diagnostic S.E.T.” I refer to these as the diagnostic “set” because theses 3 aspects all go together. These 3 items include:
1) the patient’s story
2) the findings uncovered during the process of the scalp examination including trichoscopy
3) the results of relevant blood tests.
The first letter of each of the three words 1) story, 2) examination and 3) tests spell out the word “S.E.T.” - again a helpful reminder of how the information obtained from reviewing each of these 3 aspects helps solidify a proper diagnosis. I don’t have a full story and I only have a trichoscopy photos from one area and I don’t have the opportunity to review all tests …. so I am limited to some degree in my helpfulness. Nevertheless, I do think the discussion here will be helpful.
In the early stages of hair loss, nobody can tell you have hair loss. So, when people tell you they think your hair looks normal, they are being honest. You know you hair the best.
What are the Most Likely Diagnoses in this Case?
We are deciding here between three situations:
1) Do you have androgenetic alopecia (AGA) and telogen effluvium (TE) ?
or
2) do you have telogen effluvium (TE) only ?
or
3) Do you have both of these conditions?
I think there is little doubt in your story that telogen effluvium has been present at some time in the past. Whether it is still present NOW (today) is a bit more challenging to say as we will see in a while. I will explain in a moment how we can better distinguish between the two diagnoses.
It’s fairly unlikely that other diagnoses like alopecia areata incognito are present this long and similarly the photos don’t really lead me to believe we’ve dealing with other diagnoses. Of course, a full examination can confidently exclude that. But it’s unlikely.
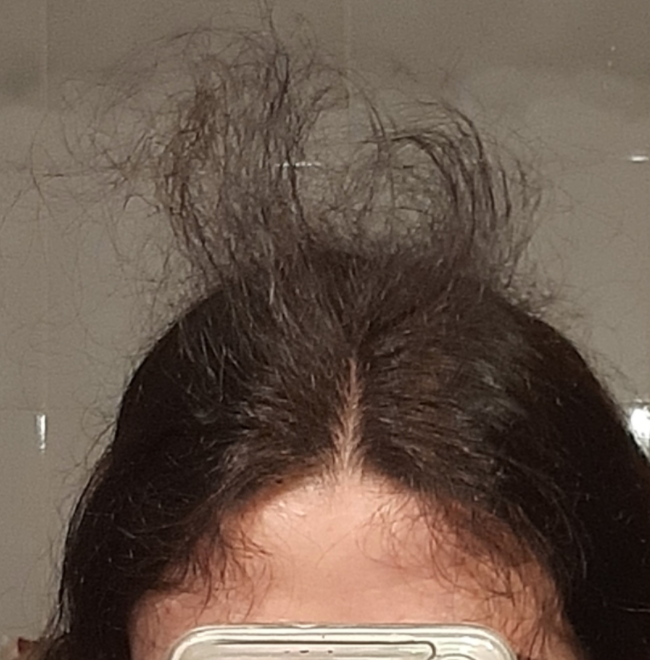
What do I see in the photos?
The photos seem to show less density ‘now’ compared to 2018. This simply tells me you have some type of hair loss. It’s true that the part width is wider in these photos but without a sense of the part width in the back (to compare to part width in the front) it would be a mistake to conclude that this widened part width equates to AGA. The temples have some subtle changes but we see these minor changes in AGA and TE. The changes in the temples do not allow me to determine the diagnosis.
The trichoscopic images you have included here are great quality. However, I don ’t know where on the scalp they are from. It’s really important when fully interpreting trchoscopy to know where the images are from.
Trichoscopy IMAGE 1
The top image appears pretty normal. Is it from the back of the scalp from more posterior regions on the head? Hairs in the first image are grouped in groups of 3 and 4 hairs. There are really no single hairs. There is slight variation in caliber of hairs but this is just a few percent that show this. It is nowhere near the 10-20 % variation in caliber of hairs that’s needed to make a diagnosis of AGA. There are no upright regrowing hair seen. The scalp is pretty healthy other than than some minor redness.. There is a bit of scale but that’s what a scalp looks like.

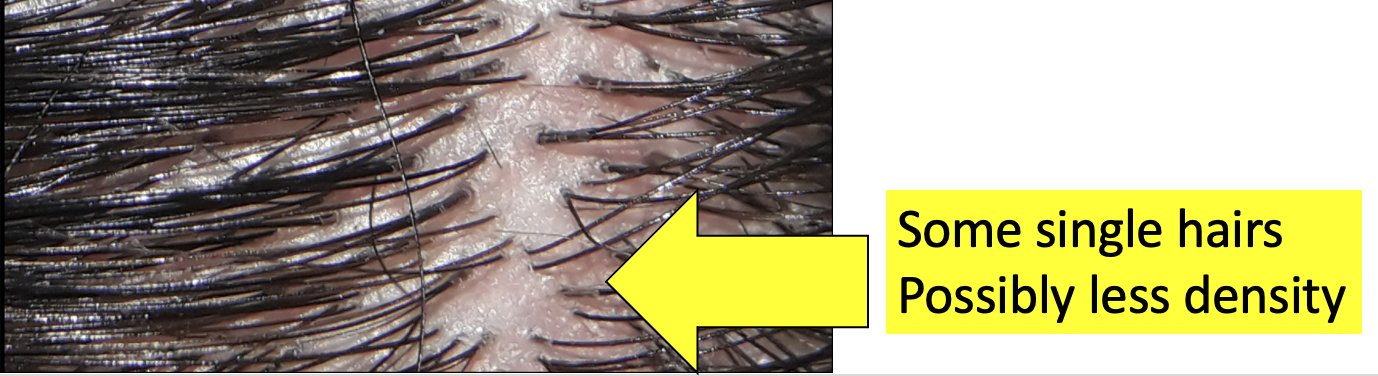
Trichoscopy IMAGE 2
The second image is different than the first which makes it important to know where exactly where it’s taken from. Whenever we interpret trichosocpy we need to know where it’s taken from or else we can’t say all that much. What stands out to me in image 2 is that it’s slightly different than image 1. This could be important but again I would need to know where on the scalp it is from. There are more single hairs seen in image 2 and the density is subtly less compared with image 1. If image 2 was from the front of the scalp and image 1 was from the back I’d be of the opinion that there was at least some good evidence for androgenetic alopecia. But I don’t know where these were taken from so I can’t say very much. However, the fact that the two images look slightly different makes me wonder about pattered hair loss - the most common being andrgoenetic hair loss.
Key Questions I Would Want to Know and Why I Would Need this Information
There is lots more to your story that I need to know if order to help determine the diagnosis in a convincing way. We need to determine if there is evidence for androgenetic alopecia and we need to determine if there is evidence for a telogen effluvium. I would want to know the answers to the following questions::
PART 1: IS THERE EVIDENCE TO SUPPORT A DIAGNOSIS OF ANDROGENETIC ALOPECIA?
Q1. Where does it feel the thinnest?
It would be helpful to know from your perspective where the hair feels the thinnest. Does it simply feel thinner “all over” (diffusely) or does one area of the scalp feel more than another? Most patients with classic TE feel that the hair is thinner all over and can’t usually point to a single area that is thinner (EXCEPT maybe the temples). In AGA, the central scalp often feels a bit thinner although some women do have a diffuse pattern or loss.
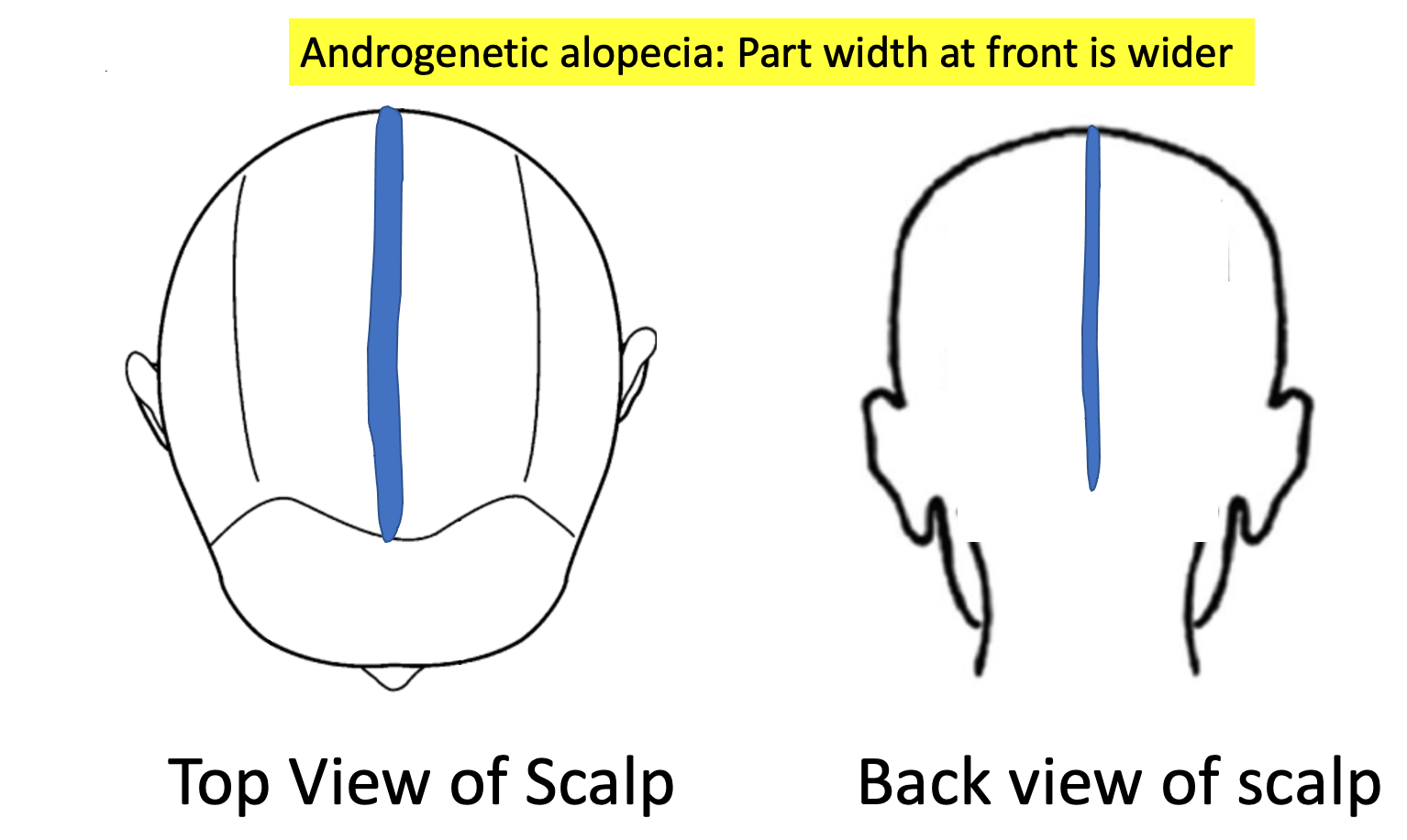
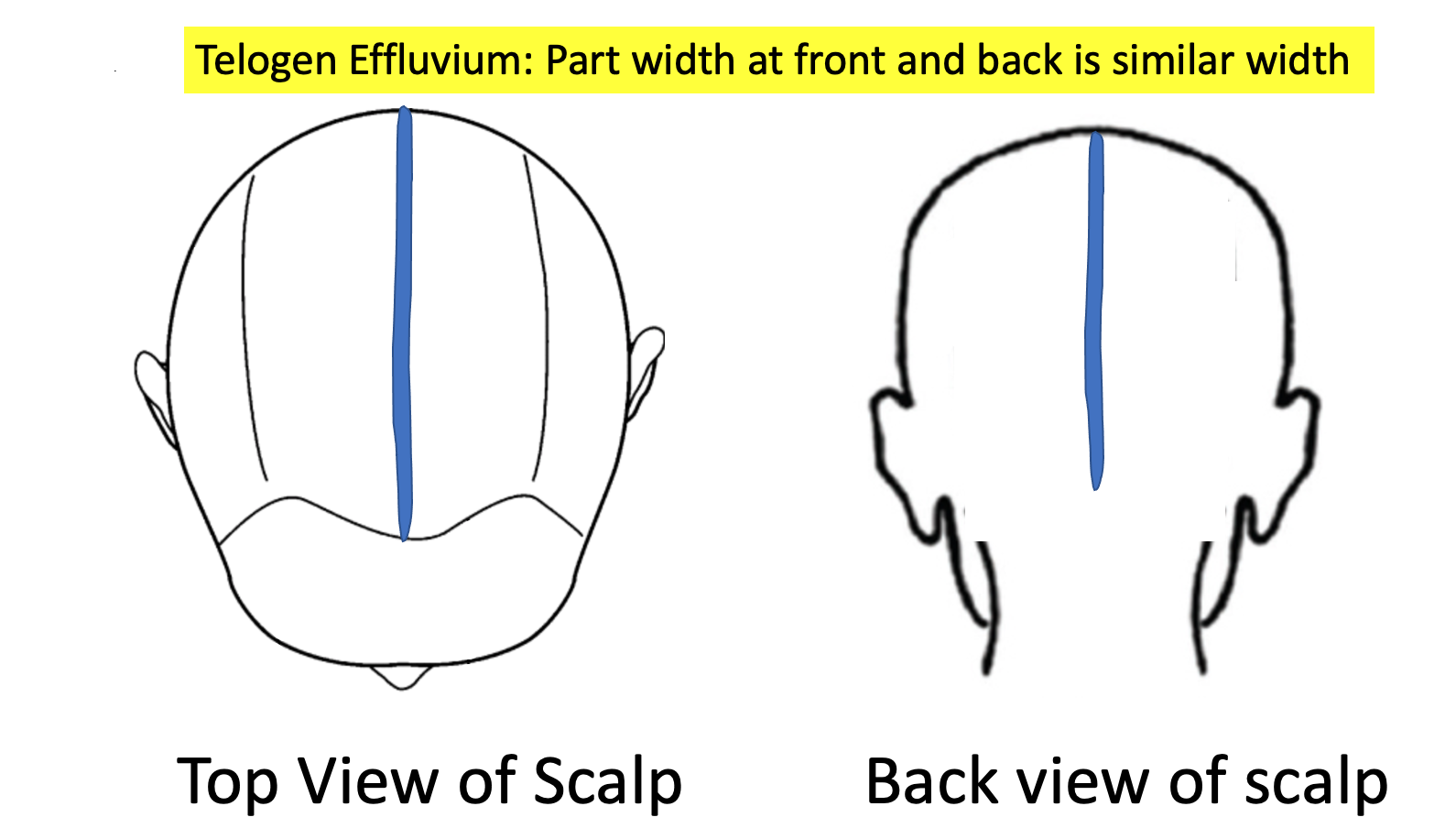
Q2. Is the part width similar in the back of the scalp as it is in the front of the scalp?
Why do I need to know? Le't’s talk now about the physical examination of the scalp and the steps your doctors would take when examining the scalp. it’s critical to know if the part width in the frontal region is the same as in the back or whether it’s different. You’ve shown a very good photo of your central part in the FRONT which allows me to see that there is more hair loss than 2018. However, what I am not able to tell now is what the part in the BACK OF THE SCALP looks like. If it’s quite similar “width” to the frontal region, that’s not really very supportive of AGA and is more supportive of TE. However, it it’s clear that you have lost more hair in the frontal region that would be more consistent with androgenetic alopecia.
Q3. What was the exact timing of starting minoxidil ?
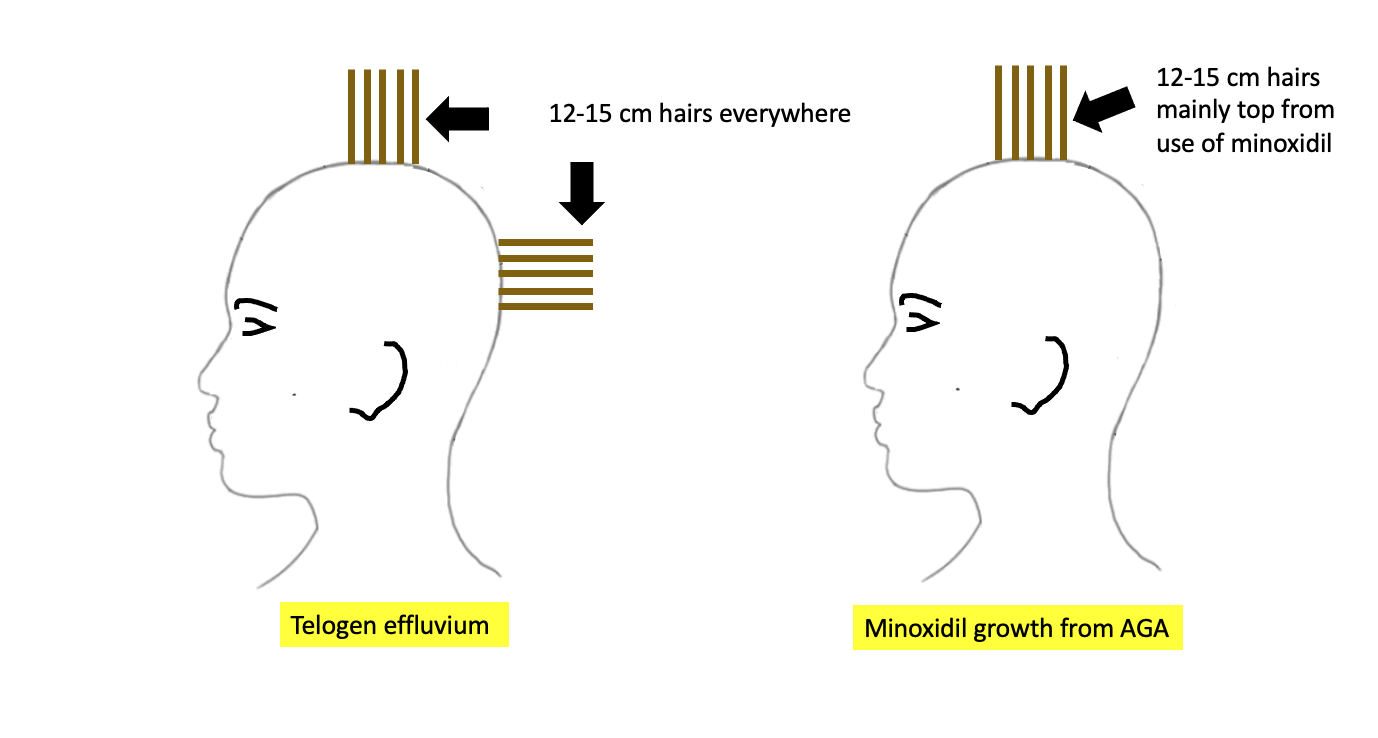
Why do I need to know? There is evidence of regrowth on the scalp. As I see in the photos, there is considerable growth of 12-15 cm hairs which means that these hairs in the middle of the scalp started growing well about 1 to 1.5 years year ago. It would be helpful to know if this is where minoxidil was applied and if it was late 2019 rather than early 2019 that minoxidil was started.
Q4. Is that 12-15 cm regrowth seen just in the middle of the scalp or is that seen everywhere equally.
Why do I need to know? When your doctors examine the scalp, it’s going to be really important to determine if this growth of these hairs is truly everywhere or just I the central scalp where I imagine you would be applying minoxidil. If the hair regrowth is just central and these 12-15 cm hairs are not found so easily in the back of the scalp, then it’s more suggestive of an early androgenetic alopecia that is present that is responding well to minoxidil.
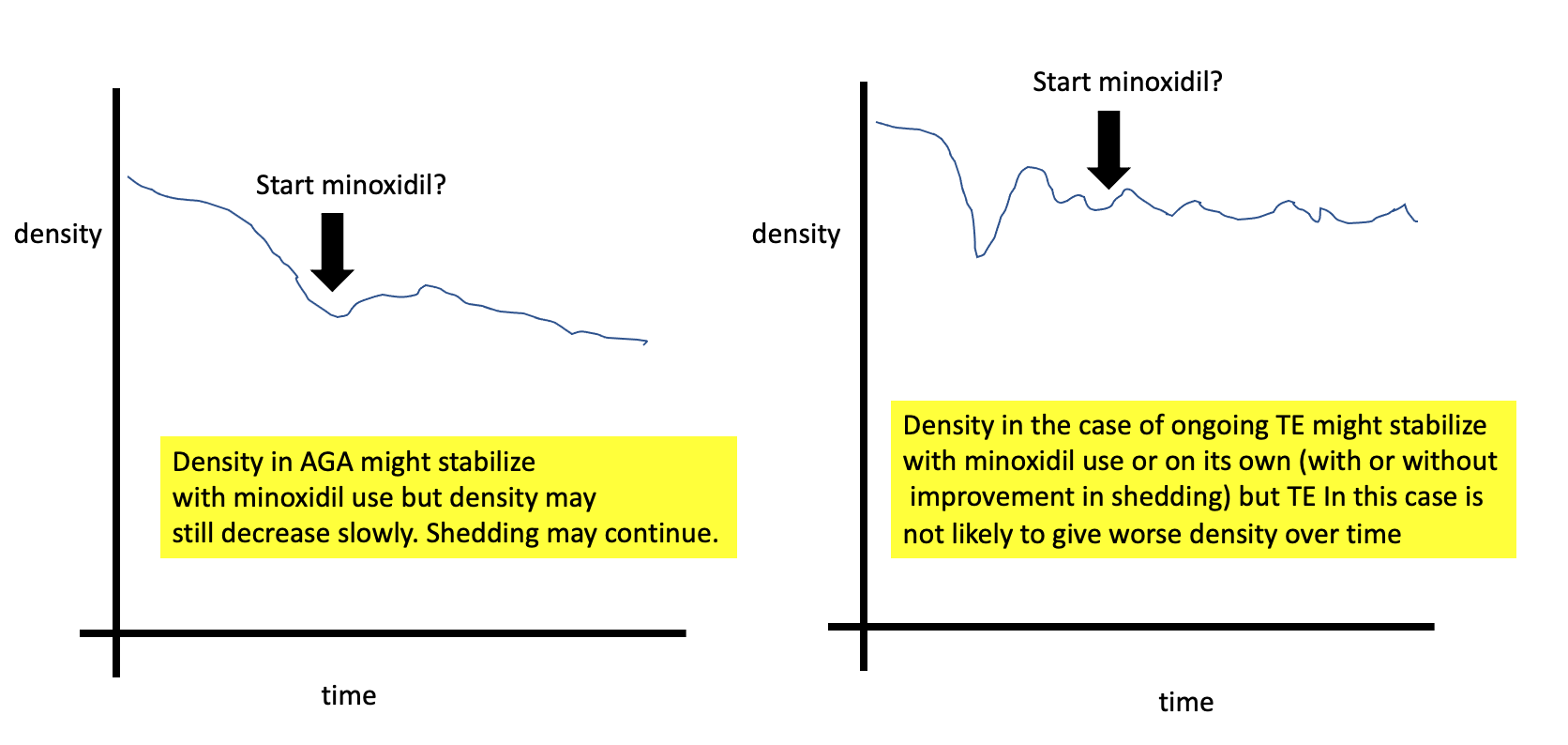
Q5. Is the hair density today less than 1 year ago or about the same as one year ago?
One of the most important questions in this case is whether or not you are still losing hair density. Here I am not referring to shedding but rather density and how thick your hair feels overall. Is it less thick? …. or just as thick as it used to be. I understand that you are still shedding but that is a bit different from whether you are still losing density. If you are still losing density and you feel that you have less hair on your scalp today than 1 year ago, that would be slightly more suggestive of possible AGA than TE. If you are still having problems with shedding but don’t actually feel your density is getting less and less, then TE still remains a very likely diagnosis.
Q6. Do you have acne or excessive hair growth elsewhere?
As we evaluate hair loss, it important to get a sense if there are clinical signs of hyperandrogenism (high androgens). Having hyperandrogenism does not necessarily mean the patient has AGA but does increase the odds just that much more.
Acne and hirsutism are two of the more important signs to enquire about. If there is any clinical evidence of hyperandrogenism, it will be important to have blood tests for testosterone and DHEAS. Only 10 % of women with AGA have hyperandrogenism so the finding of normal hormone levels still makes AGA possible. In addition, many women with hyperandrogenism do not have AGA at all so this is just a fact that gets considered as part of the bigger picture.
PART 2: IS THERE EVIDENCE TO SUPPORT A DIAGNOSIS OF ONGOING TELOGEN EFFLUVIUM?
It’s clear that a telogen effluvium was present in the past for you. The key question now is whether there is some kind of ongoing TE. The causes of telogen effluvium include stress, low iron, thyroid problems, medications, diets, systemic illness. So we need to understand more about these potential issues or ‘triggers’ for anyone who is shedding. In CTE, shedding can occur without a clear trigger.
Q7. Did you start and stop other medications or supplements?
Why do I need to know? Other medications and supplements can trigger shedding. Even taking some medications and herbal medications can give an ongoing shedding. I’m assuming in this scenario that minoxidil is the only product used. Clearly, if other products are used they need to be considered.
Q8. Have you had eyebrow changes, eyelashes changes, body hair changes, nail changes?
Why do I need to know? Eyebrow and eyelash changes and body hair changes don’t occur as part of AGA but can occur in TE. They can also occur in other immune based conditions. I am not suspecting any immune based issues but certainly it would be quite unexpected if you were experiencing a lot of body hair loss. If there was any eyebrow or eyelash loss, the key is to figure out if it affects both the right and left side symmetrically or whether one side is affected more. Eyebrows and eyelashes can reduce in density from telogen effluvium, alopecia areata, trichotillomania, seborrheic dermatitis as well as cicatricial alopecia (and other conditions). It would not be surprising if you have some minor eyebrow changes over the last 3 years but it should be quite symmetrical. If you do have eyebrow changes, some of the eyebrow changes could be due to the hypothyroidism.
Similarly, if there was an increase in body hair this too would be unexpected here and a possible sign of increased androgens. Increased hair on the thighs, abdomen and nipples can be a sign of hyperandrogenism and raise suspicions for PCOS (even if periods are regular). I would think that it issei's quite unlikely you would report this to be the case. This would be information that your doctors should confirm.
Q9. Have you had weight loss or weight gain? What is the current weight?
In the setting of a likely telogen effluvium, it’s important to know whether there has been weight loss that could be triggering a telogen effluvium. In addition, we need to make sure that your current weight is high enough (i.e. BMI is above 18) otherwise the result can be an ongoing TE from poor nutritional status.
In addition, weight loss and weight gain can be reflective of underlying medical conditions. So, if weight has fluctuated either way, it could be important.
Q10. Do you have any scalp itching, burning or tenderness?
Scalp symptoms are important to know for every single patient. Your scalp looks quite healthy so I would be surprised to learn there is any itching or burning or tenderness. I’m usually not too worried about a slight among of itching from time to time, but if there was burning or tenderness in the scalp, that would be worrisome. I don’t think this is very likely to be relevant here for your case but we need to always keep in mind that there are conditions that mimic telogen effluvium.
Q11. Do you feel you are getting hair breakage?
I am not appreciating much in the way of hair breakage, but it’s important to inquire about. Some patients confuse hair breakage with actual new growth so what you are seeing on the top of the scalp appears to be new growth. It’s not uncommon for patients to exclaim - “look at all my hair breakage!” In your case, this is not breakage from what I can see. However, if you felt there truly was increased breakage that would need further exploration. Breakage can come from heat and chemicals and can give the feeling of ongoing shedding and loss. A proper examination can completely exclude breakage, but I would be surprised if that’s even an issue here. your scalp and hair are healthy.
Q12. How low your ferritin dropped over this period ?
I understand that you have a history of low ferritin. It will be important to know what your ferritin level is right NOW. That is what will be relevant to ongoing shedding. A ferritin of 10 is likely associated with hair loss. A ferritin of 40 is probably not. Therefore, it will be important to know what the ferritin level is now and how it’s been changing over the last few years.
is it possible you’ve had a ferritin of 22 and it’s been responsible for your shedding for three years? Perhaps. The higher your ferritin level - the less likely it is that your iron is the culprit in your hair loss. But you have not given me the number so I don’t know the current level.
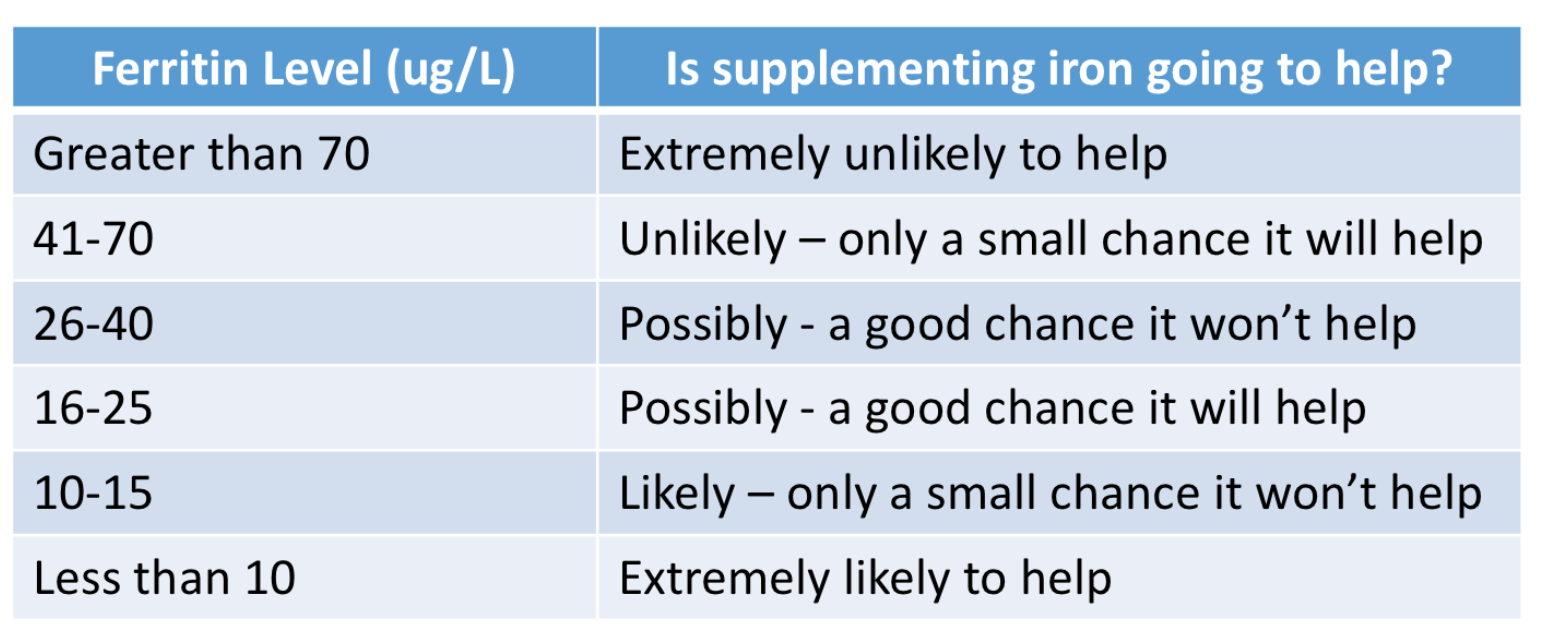
Certainly, if you have a ferritin less than 15, it’s probably a problem and probably one of the reasons why your hair is shedding. Taking iron supplements in these situations has a high likelihood of helping. However if your ferritin is currently 40, 50 or 60, it’s less likely that you currently have an iron problem.
Most women need ferritin levels in the 30-40 range for healthy hair. However, some women definitely need those levels to be higher than that and into the 50 - 70 range. If you have a history of low ferritin, it will be important for your doctors to review why you have low ferritin and how the levels have been changing over time and what they are now. Many women have low ferritin levels. However, when low ferritin is combined with low hemoglobin (which we call iron deficiency anemia) I’m much more concerned. Excessive bleeding from menstrual cycles, poor diet, celiac disease, gastrointestinal issues all need to be explored.
The following table gives an estimate of how likely it is that taking iron supplements will help your hair according to the ferritin levels.
Q13. When did you start thyroid medications? Have your thyroid levels (TSH) changed during this time? What is the exact reason for the thyroid disease (Is it autoimmune Hashimoto’s?)
It would be helpful to understand when your thyroid disease was diagnosed and whether the TSH has been changing over this period. Some patients occasionally have fluctuation TSH levels which give shedding. Also, it would be important to know if you are on thyroid medications NOW and when this started and whether the dose has been changing over time. It is important to know the exact causes of the thyroid disease.
Q14. Were your periods always regular?
It’s always reassuring to know that your periods are regular at the present time. It would be important to know if they have always been regular of whether they have become regular just recently. It would be important to know exactly what each patient means by regular periods. Are some cycles considerably longer and some shorter than others? Having regular periods does not make it impossible to have an endocrine issue but does make it less likely. Having regular periods does not necessary mean these are ovulatory cycles but for most women they, of course, are. ovoluatory cycles.
Q15. Has your density ever come back to normal or has it just become less and less?
It would be important to know whether you feel your density and thickness ever came back to normal. When the shedding stopped for four months, did density return? Do you know the reasons why the shedding stopped for those 4 months? Was it that your iron levels finally came up? Was it that that your thyroid levels were brought back to normal? Was it that stress was reduced? Was that the period that minoxidil was started?
If your density did return completely to normal, this makes AGA much less likely during those times. It does not mean that it could not have happened or developed later but we would not expect your density to come back to 100 % normal in the setting of AGA.
Q16. Do you have other symptoms like joint pains, headaches, fatigue or rashes?
In situations like this, it’s helpful to know if the patient has any other symptoms that could suggest a systemic cause for a telogen effluvium. Issues like going pains, chronic headache, unusual fatigue or rashes on the body could prompt further work up and evaluation.
Q17. What other conditions run in the family?
it’s helpful to know what conditions run in your family. I understand your mom uses minoxidil so that tells me there is a family history of AGA. It’s helpful to know what the hair density is like in other males and females in your family. It’s also helpful to know what other diseases or medical conditions run in the family. These would include issues like psoriasis, lupus, inflammatory bowel diseases, arthritis, alopecia areata, diabetes, multiple sclerosis, early menopause, infertility and polycystic ovarian syndrome.
What Would I Recommend Next?
1. The answers to these questions above are going to be helpful and so is an evaluation of the frontal part width and back part width. That could be really informative in this case. If the part is wider in the frontal regions than the back, this suggests a possible diagnosis of AGA. If not, it still could be but TE becomes more likely.
2. Comparative trichoscopy of the middle of your scalp compared to the back of your scalp is going to be very very helpful in reaching the proper diagnosis. If the two are really different with more single hairs in the frontal and more variation in caliber noted in the frontal regions, then AGA becomes a likely diagnosis.
3. Current blood tests from ferritin and TSH and CBC are going to be important. I suspect you’ve had these tests done many times. If your ferritin is not high enough, it could be that you are shedding chronically in part from iron deficiency. The history will guide if other blood tests are helpful.
4. Finally, 5 day modified hair wash test (MHWT) is likely going to be the most helpful and least invasive next steps. Of course, a scalp biopsy can also be done but I think a modified hair wash test is probably going to be better in this case. The five day MHWT is fairly easy to do and you can do it yourself at home if you are so motivated to do so. The hair must not be washed for five days before doing the test. A 5 day modified hair wash test (MHWT) is a standardized means of assessing and quantifying hair shedding and provides information on the type of hairs being shed. It is a non-invasive method to measure hair loss by counting and identifying rinsed out (shampooed) hairs. To begin the test, a gauze is placed in the sink and hair is shampooed normally and the hair is rinsed in order to collect and trap all shed hairs on the gauze. The hair can be shampooed and rinsed repeatedly in order to remove all hairs that need to come out.
The following is helpful diagram illustrating the key steps in the 5 day hair collection.

After gently lifting the gauze from the sink, the gauze is then dried for 3 days and then counted. In our clinic, patients who do this test mail the hairs to us, but patients can also go about counting hair. It is important that the gauze not be disturbed while drying or mailing as this gauze has dozens of small fine barely detectable hairs that must be included in the analysis. The final number of hairs as well as the proportions of 3 cm or less hairs, provides information on the relative proportions of androgenetic alopecia as well as telogen effluvium. The proportion of broken hairs and the proportion of abnormal hair gives us a sense of the possibility of an autoimmune issue such as diffuse alopecia areata.
The number of hairs collected in the MHWT can give a good sense of excessive shedding. Ideally, results need to be interpreted by a dermatologist who is familiar with the performance and interpretation of this test but as mentioned patients can count hairs.
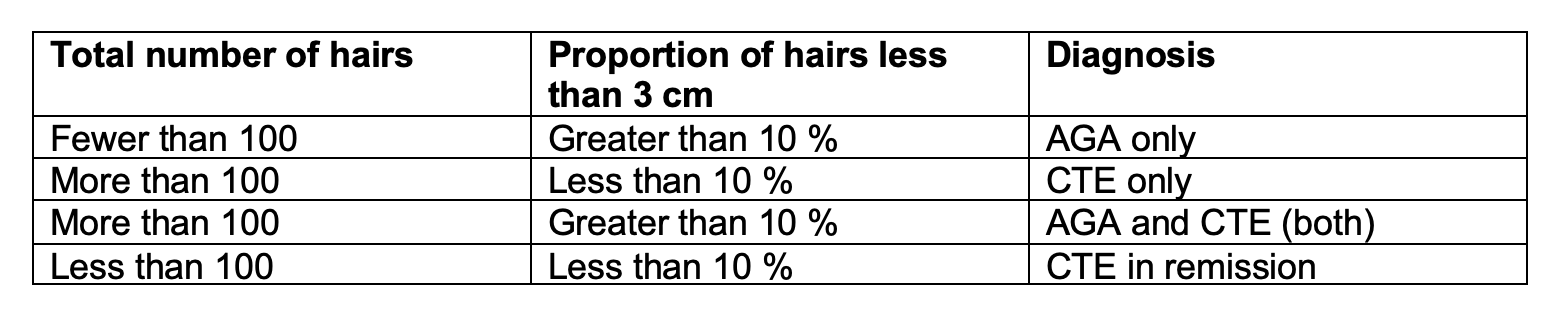
a) Patients with 10% or more of hairs 3 cm or shorter and who shed fewer than 100 hairs are diagnosed as having androgenetic alopecia (AGA).
b) Patients with fewer than 10% of hairs that were 3 cm or shorter and who shed at least 100 hairs are diagnosed as having chronic telogen effluvium (CTE).
c) Patients with 10% or more of hairs that were 3 cm or shorter and who shed at least 100 hairs are diagnosed as having AGA + CTE
d) Finally patients with fewer than 10% of hairs that were 3 cm or shorter and who shed fewer than 100 hairs are diagnosed as having CTE ‘in remission.’
Final Summary
Thanks again for sending in your question. I hope this was helpful. A few more details in this history together with a good scalp examination is going to go a long long way here in getting to the correct diagnosis (or diagnoses in the event there are two).
IFor you, I think that a 5 day modified hair wash test is going to really help give the evidence that you need to move forward with the right diagnosis. If there is any doubt, then a biopsy could further clarify but I doubt it will be needed.
The use of minoxidil could complicate things a bit in this case but only slightly. If one were to stop minoxidil and find that significantly worse shedding happens 4-6 weeks later I do think this would also be proof of some component of AGA being present.