What can I use for my eyebrow alopecia areata?
Can I use clobetasol on my eyebrows? I don’t want steroid injections!
I’ve selected this question below for this week’s question of the week. It allows us to review some concepts in treatment of eyebrow alopecia areata.
Question
Hi Dr. Donovan. I’m a 28 year old male. I have alopecia areata and have had patches on my scalp for a few years. I’ve been able to get it back with steroid injections and clobetasol. I’m losing eyebrows now and really freaking out. I am scared to get injections as I always faint and pass out. I know it’s silly but I’m having trouble getting myself to this stage. Can I use clobetasol on the eyebrows? It’s been helpful for the scalp but the dermatologist says no. I think we’re now running out of treatment options.
Answer
Eyebrow alopecia areata is treated differently than scalp alopecia areata. First, the eyebrow area has thinner skin than the scalp skin, so potential local and systemic side effects from treatment are different. Second, the area is close to the eye so effects on the eye need to be considered. Clobetasol is too strong for the eyebrow skin!
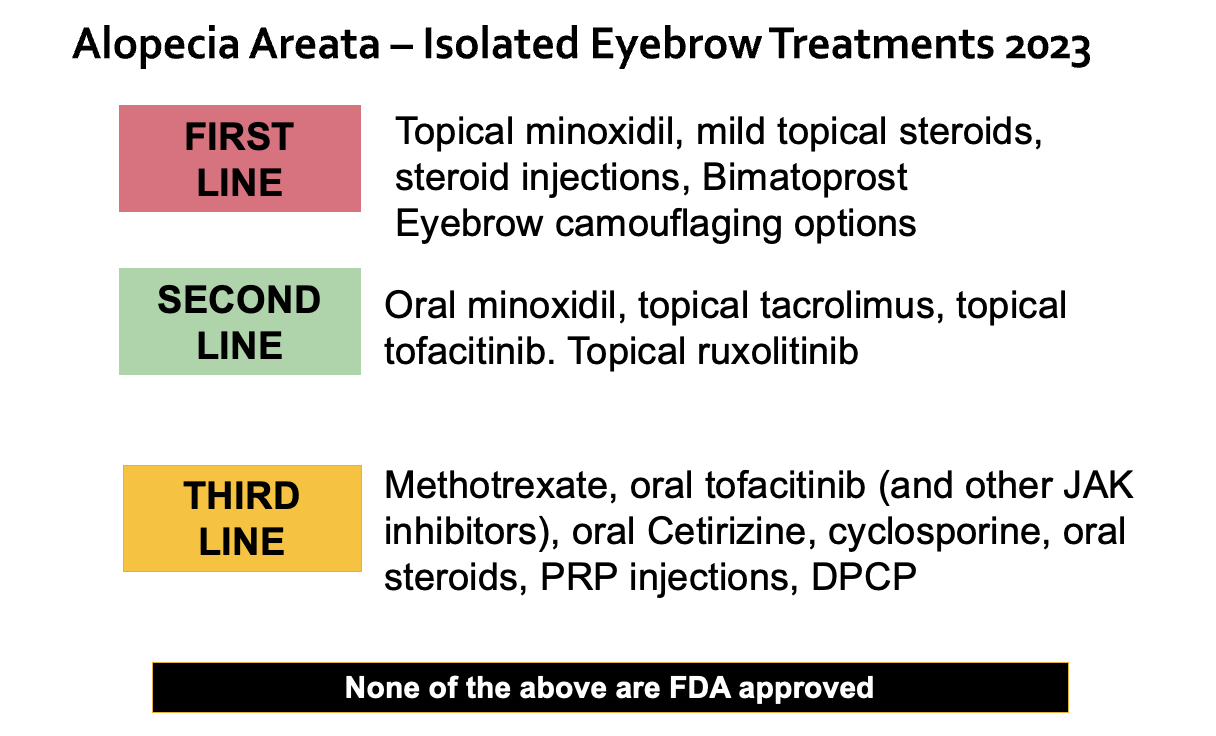
There are a large number of potential treatments as outlined in the image above. First line treatments for eyebrow alopecia areata include topical minoxidil, topical steroids, steroid injections and topical bimatoprost (Latisse). Steroid injections are most effective but injections do not help everyone and can be quite painful for some patients. (It would not be a consideration in a small child but we have performed steroid injection in patients as young as 15 years).
I understand your worries about the eyebrow injections. There are things that help alot including lying the patient down flat on a pillow when the injections are done and having it done by someone with a lot of experience who can puncture the skin quickly and with less pain. iI’s all over in 40 seconds. That said, I still understand that this is not the right treatment for everyone.
Typically, treatment for alopecia of the eyebrow starts with topical minoxidil in the morning and mid potency topical steroids (like fluocinonide gel) in the evening for four weeks. As mentioned, a strong steroid like clobetasol is not generally appropriate for use on the eyebrow (there are exceptions where very short courses may be). After the four weeks is up, minoxidil continues nightly and fluocinonide is reduced to three times weekly for two more weeks.
If there is good growth, and it appears things are on track, I may continue minoxidil daily and slowly reduce fluocinonide gel to twice weekly for two weeks and then once weekly for two weeks and then stop. Minoxidil may be continued in most cases until eyebrow density has been stable for a long time. Side effects need to be monitored by a physician knowledgeable about these treatments.
Once eyebrows have grown in, the minoxidil too will be stopped.
Eyebrow alopecia areata often is associated with a tougher to treat and more resistant alopecia areata, so it’s quite likely for further hair loss to occur at some point. The same protocol can be started up again if patches occur.
What is eyebrows don’t grow with minoxidil and fluocinonide gel?
If eyebrows are not responding well to minoxidil and fluocinonide gel after the first four weeks, then I will revisit the possibility of doing steroid injections with my patients. The answer still may be no, and that’s okay. But if yes, injections can be done every 6-8 weeks with 2.5 mg per mL triamcinolone acetonide with 6-7 little injections per brow (assuming complete loss). Smaller patches require fewer injections. If not responding well, I may increase to using 5 mg per mL of the triamicinolone medication. Side effects like atrophy need to be discussed with the patient as a dimple in the eyebrow skin, while temporary, can be disfiguring and extremely concerning for patients.
If injections are not desired, or the physicians is not comfortable performing them, then one may move on to topical minoxidil in the morning and Bimatoprost in the evening. Bimatoprost is sold under the trade name Latisse. This routine can be continue daily for 8 weeks before re-evaluating response.
If there is good growth, then minoxidil can be continued daily and Bimatoprost can be reduced to three times weekly for 8 more weeks before deciding on whether to reduce further two 2 times per week. I likely would continue twice weekly long term (6-8 months or more) but this is evaluated on a case by case basis.
If minoxidil, fluocinonide and Bimatoprost are not helpful and steroid injections are not possible OR if they are only partially helpful I will consider adding oral minoxidil or a topical JAK inhibitor.
Oral minoxidil would be a first step and together with topical minoxidil and topical bimatoprost and/or topical tofacitinib (which we’ll review below) …. these treatments can be really helpful. Doses of oral minoxidil are 0.625 mg to 1.25 mg daily for adult female patients and 1.25 mg to 2.5 mg in adult male patients. Higher doses are possible on a case by case basis and some males increase to 5 mg daily. The requirement for oral minoxidil signals a more resistant and tougher to treat form and the expectation should be that this treatment will be needed 9 month to several years. Side effects, as for all treatments discussed above, need to be carefully reviewed and consent obtained. These include hair growth on the face or body, fluid retention, heart palpitations, fatigue, chest pain. Medications are contraindicated in pregnancy for female patients.
Topical JAK inhibitors are a good second line option as well. A compounding pharmacy can make 2 % to 2.5 % topical tofacitinib creams, foams and lotions and topical ruxolitinib ointment is commercially available in the United States (although it is only available as a greasy ointment). The topical JAK inhibitor drug can be applied once to twice daily. The decision on whether to use once or twice daily will depend on the response to the treatments in the steps above. Complete failure to regrowth eyebrow hair with topical minoxidil and topical fluocinonide gel may prompt me to consider twice daily topical JAK inhibitors and abandon other treatments.
Options if Topical Steroids, Steroid Injections, Topical Bimatoprost and Topical Tofacitinib Don’t Work:
If hair does not respond to topical options or steroid injections, strong consideration can be given to oral steroid pulses, oral methotrexate or oral JAK inhibitors provided there are no contraindications. These may or may not be covered (reimbursed) by drug plans depending on the amount of scalp hair loss. (Many insurers look to the amount of scalp hair loss when deciding on whether to reimburse for medications). A decision to use these therapies should be done with the understanding that treatment may be needed long term, and possibly lifelong.
Finally, I want to tell you one of the greatest secrets ever for helping patients to avoid passing out. It involves drinking an entire 300 mL bottle of cold water quickly 1 minute before getting injections done. It has to be consumed fast and it has to be cold (ideally). I would say that it has reduced fainting in fainters by 80 %. It works incredible. Consider it before you get your blood tests and if you do go for injections - before your injections too.
Conclusion
I thank you for your question. I hope this helps you in your discussions with your own doctors. There are many options to consider so be sure to review them all thoroughly with your doctors. It’s okay to feel one of the options is not right for you but be open to revisiting the options over time. It could be that one option does not feel right now but could feel right in the future.