Dose of Finasteride for Frontal Fibrosing Alopecia in Males
What is the correct dose of finasteride for treatment of male FFA?
I’ve selected this question below for this week’s question of the week. It allows us to review some concepts related to the correct dose of oral finasteride for treatment of male frontal fibrosing alopecia (FFA).
Question
I have a very simple question which I cannot find an answer for anywhere...maybe that means it isn't so simple! The use of finasteride and dutasteride for those with FFA is well known. Many studies refer to finasteride doses of 2.5mg or 5mg daily, but all seem to be for women. For men with FFA already using 1mg finasteride daily for androgenic alopecia, should they up their dosage to 2.5mg, or even 5mg per day? I can't find anything, any study, any reference anywhere that answers this question.
Answer
Many thanks for this question. This is a great question! You’re right - it’s not something that really gets looked at carefully in the research world. When you actually look at all the research papers on male FFA, most talk about things other than treatment! These research papers are filled with detailed information on patient age, where the hair loss occurs (eyebrows, scalp, beard), and other medical conditions affected patients have. It’s so incredibly rare to find good information about treatment (especially detailed investigations about finely tuned dosing!)
There has never ever been a good study examining 2.5 mg finasteride compared to 1 mg finasteride in males with FFA.
Now, that said, there is no good reason to believe that 1 mg is a problem. Many of my male patients are using 1 mg finasteride … and see benefit!. Would 5 mg be better? There is no reason to believe so but again studies have not been done. Petersen and colleagues (reference below) described a study of 7 male patients with FFA. 3 were put on oral finasteride and those three ended up staying on finasteride because it was part of a plan that helped.
Alegre-Sánchez and colleagues (see reference below) described 12 males with FFA. Just one was put on finasteride … and it helped.
So in most studies we have patients that are put on 1 mg finasteride stay on 1 mg finasteride.
Discussion and Conclusion.
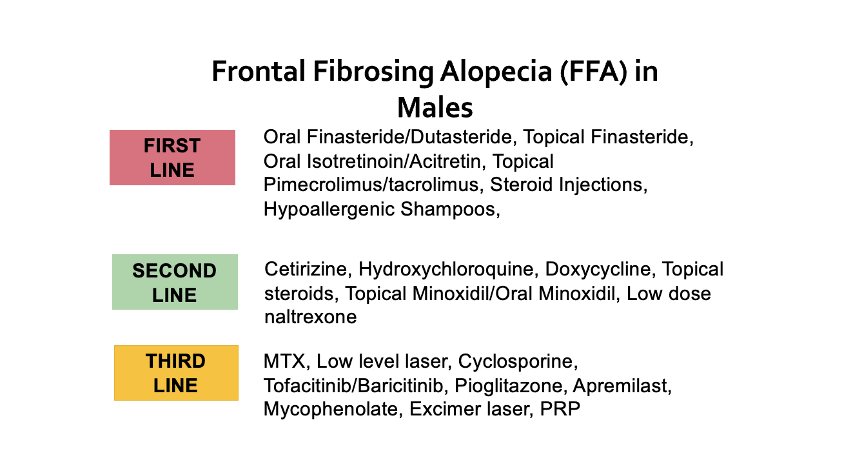
Your question is a great one and the reality is that the studies of FFA in males are few and those that we do have show patients with a wide variety of treatments. I’m not so sure that FFA in males is so so so “antiandrogen responsive” like female FFA. It certainly is to some degree - but until that time we learn more I think it’s reasonable to cover the bases with prescribing antiandrogens PLUS other immune modulators (doxycycline, and other tetracyclines, hydroxychloroquine, steroid injections, topical calcineurin inhibitors (pimecrolimus) and/or retinoids like isotretinoin.
It really all comes down to getting on a solid plan that a person is comfortable with and then taking incredibly good photos every 3-6 months. If the photos look the same (and I mean 100% the same) then that means the disease is coming under good control.
If there is evidence of loss, that’s where I would switch a patient who is using finasteride 1 mg to dutasteride 0.5 mg (or go up to 5 mg finasteride if dutasteride is not an option for some reason).
Now that said, we don’t have any great evidence to support finasteride over dutasteride in males with FFA quite yet. In females, oral dutasteride does seem to be the favourite option for FFA. We just don’t have the data in males. So there’s nothing wrong with oral finasteride 1 mg for treating FFA in males. Lots of data supports it.
I think other things need to be considered as well. If there is evidence of ongoing beard and eyebrow and eyelash loss, then I probably would bring on board some good antinflammatories as mentioned. Hydroxychloroquine, isotretinoin, cetirizine, isotretinoin, methotrexate, and JAK inhibitors are on that list.
If I see a patient with new FFA in the clinic, I generally start 0.5 mg dutasteride rather than 1mg finasteride. This is not because there is good evidence in males but because it seems to be the preferred option in females. If I see a patient who is already on 1 mg finasteride and doing well, I may continue it for the time being and optimize other parts of the plan before thinking about a switch to dutasteride.
Good photos are key. The photos don’t need to be done weekly but rather every 3 months. If hair is continuing to be loss, then one needs to shift gears and change the plan.
REFERENCES
Alegre-Sánchez A et al. Frontal fibrosing alopecia in male patients: a report of 12 cases. J Eur Acad Dermatol Venereol. 2017 Feb;31(2):e112-e114.
Peterson E et al. Frontal fibrosing alopecia in males: demographics, clinical profile and treatment experience. J Eur Acad Dermatol Venereol. 2020 Feb;34(2):e101-e104.