Frontal Fibrosing Alopecia (FFA): Is there a case for preventing further loss?
Frontal Fibrosing Alopecia: Can Further Hair Loss be Prevented?
I’ve selected this question below for this week’s question of the week. It allows us to review some concepts related to treating frontal fibrosing alopecia (FFA).
Question
I have been dealing with a slow onset of hair loss for the past two years. The loss frames the front of my face, otherwise, I have very thick hair in the back and quite a bit still on the sides. It’s mostly from the top of one ear around to the other. I am a 67 year old female. I am hypothyroid. My mother also had frontal hair loss. She was never diagnosed with anything. I attempted to have a transplant and the professionals at that office told me just from appearances of hair loss, and eyebrow complete loss, that I was suffering from frontal fibrosing alopecia. I have read so many stories of different treatments from different patients and have come to the conclusion that with FFA there is really nothing that’s going to bring my hair back but is there a case for preventing further loss? I am currently using oral and topical minoxidil. I also take 5000 mcg biotin per day. I used spironolactone for about nine months but really saw no measurable change so I have stopped taking that. I am simply now trying to save my hair and prevent further loss. I don’t have any redness or itching.
Answer
Thanks for the question.
In 2023, we not only are able to stop FFA in a good proportion of patients - but we improve the hair density in some patients with FFA as well. Now, we might not get the right combination of treatments on the first try and sometimes not even on the second try. But in 60-70% of patients. we’ve either halted the disease or improved it within 18 months of diagnosis. Usually much sooner. Unfortunately, not every single patient will have their disease stopped - but a very large proportion do.
Let me start our discussion by sharing a photo from a 2015 paper titled Finasteride-mediated hair regrowth and reversal of atrophy in a patient with frontal fibrosing alopecia. You can see in the image a patient with FFA that not only had her disease stopped but had improvement. Granted, this does not happen to every single patient but it happens way more often than people realize. And so does halting of the disease.
Of course, this happens more often if the right treatments are administered. We’ll get to that in a minute.
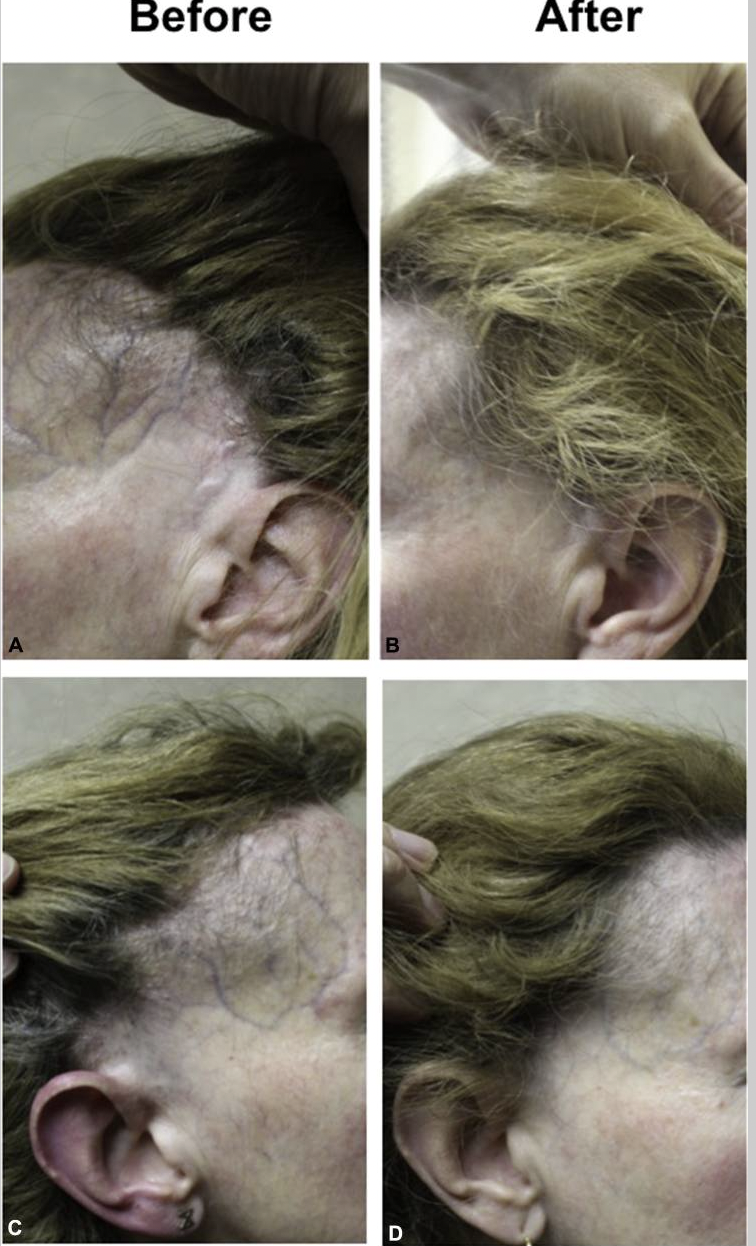
Hair regrowth and reversal of atrophy in a patient with frontal fibrosing alopecia. A and C, Before introduction of finasteride. B and D, 12 months posttreatment with finasteride, 2.5 mg. Note hair regrowth and reduction in atrophy. from Donovan J. Finasteride-mediated hair regrowth and reversal of atrophy in a patient with frontal fibrosing alopecia. JAAD Case Reports 2015
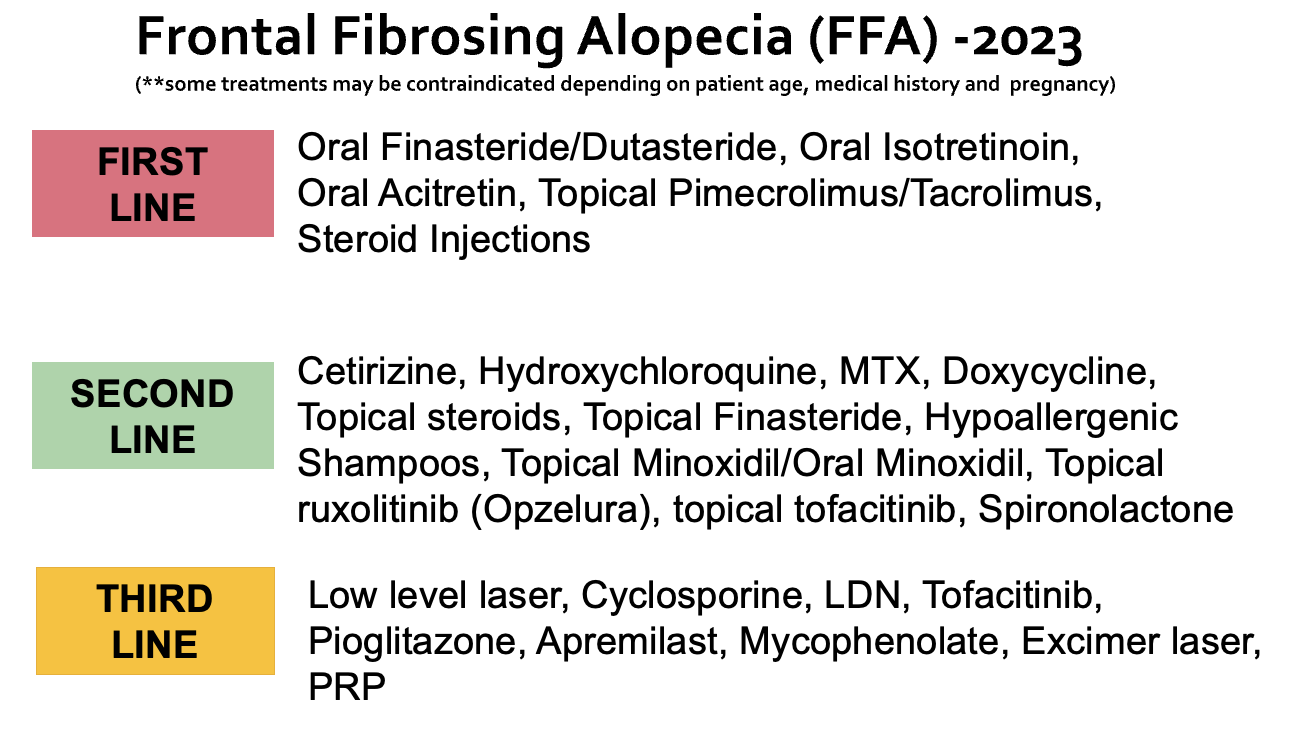
The “GOLD SLIVER AND BRONZE” FFA Treatments.
As many people know, I often refer to treatments that one can choose for any disease in three categories. These are the “gold”, “sliver” and “bronze” categories. Now, physicians sometimes call these categories first line, second line and third line treatment categories but I like to call them gold, silver and bronze.
Gold treatments come with the highest chances of halting the disease (or improving it) or are just really reasonable options given their safety and affordability and effectiveness. If gold treatments don’t work well (or one can’t use them for whatever reasons), then one should look at whether there are any other gold treatments that can be used before finally thinking about starting a “silver” treatment. One should consider one or more silver treatments as the next step. And if silver treatments don’t work (or can’t be used for whatever reason), one might consider bronze treatments.
There is of course a fourth category - and that is a category of treatments that I don’t think do that much.
So here’s the list!
Now, not everyone is a candidate for every medication. So it’s not simply that one takes this list to their doctor and says “give me this medication.” It does not quite work that way. A patient with severe dry eyes may not tolerate isotretinoin. A young patient who wishes to become pregnant should never be prescribed finasteride or isotretinoin. A person with severe depression may not be a great candidate for finasteride (as it rarely affects mood).
So there are reasons why one might and might not consider certain medications - and this all needs to be reviewed with the doctor overseeing care.
But here you have it - you have the Gold, Silver and Bronze list for treating FFA!
What’s so valuable about the list?
This list gives us a framework. Patients come in the office all the time and say to me “I have FFA , Dr Donovan and nothing works! I tried rosemary oil and zinc pills and every supplement you can imagine. Nothing works! This is hopeless”
So then I look at my trusty gold, silver and bronze chart and see that nowhere is rosemary oil and zinc pills and supplements seen on that list.
So effectively, the patient has tried nothing.
and so I tell the patient - effectively you have tried nothing so far.
A Typical Patient with FFA
Not every patient with FFA starts the same treatment. I don’t really believe in cookbook recipes and templates to treat any type of hair loss. I need to understand everything about the patient and her or his past health and current medications and current treatment goals. But it would not be uncommon in a post-menopausal patient with FFA to start (after getting baseline blood tests and assuming no contraindications to these treatments) oral dutasteride 0.5 mg five times weekly with isotretinoin 10 mg three times weekly with pimecrolimus cream 3-5 times weekly on the hairline and consider steroid injections in the hairline with 2.5 mg per mL. I’ll then repeat the steroid injections in 3-4 months and follow how the patient’s hair loss is doing. I’ll take a zillion photos before starting and another zillion as we go along. If it’s clear we are winning we might stay the course with this plan. Otherwise I might increase isotretinoin and dutasteride dosing to daily and possibly bring on board treatments like oral hydroxychloroquine (Plaquenil) and/or oral cetirizine. We’ll repeat the steroid injections and I’ll see the patient back in 3-5 months.
Again, you can see that I methodically follow the gold, silver and bronze ladder of treatments. I don’t follow what’s popular or what’s new or what’s trending. I follow what’s proven to work. Now this list above changes year to year as new research confirms what works better than others and once research confirms what new treatments are useful.
The Gold, Silver and Bronze Treatments.
The Gold, Silver and Bronze List shown here is my list. Another doctor who treats lots and lots of patient with FFA will have a similar list - but it could be slightly different. It won’t be dramatically different if that doctor treats lots and lots and lots of patients with FFA. Why? Because these are the treatments that help!
If a doctor does not treat lots and lots of FFA, then yes, their list will differ quite a bit.
I often hear patients say to me “Dr So and So likes to start all patients with FFA with platelet rich plasma or PRP.”
That’s fine. That doctor is saying that his or her first line treatment is PRP. In my opinion, that’s not a first line treatment for FFA. That’s a third line treatment. There’s nothing wrong with PRP - but in my opinion it does not come with the same chance of halting the disease as what you see in the first line category.
Do I ever user PRP treatments for patients with FFA?
For the sake of discussion, let’s continue this PRP topic and ask the question “Do I ever user PRP treatments for patients with FFA?” Sure, I use every single treatment you see listed above. If you see a treatment on the list above, I use it or will refer the patient to someone who does it. Now, I don’t use them all in the same patient at the same time. But I might add PRP treatments for a patient who is doing fairly well on oral dutasteride and oral isotretinoin and hydroxychloroquine and topical pimecrolimus and needs a bit more help to get this disease shut off. We’ll add PRP to the plan!
Do I start PRP as the first treatment? Not usually, no. But of course, if a patient says to me “I’ve listened to all your gold and silver treatments and I don’t want them right now. I want to start PRP first and then we’ll take it from there.”
What might I do?
Well, I’ll tell the patient that I support their decision and I’ll also remind the patient that other options probably will give a better chance of helping but provided the patient is informed - I’m okay with that plan!
Conclusion
Thanks for your question. In short, there is a case for preventing hair loss! But there is so much more. Some patients with FFA actually get improvements too - so that’s not an impossibility.
I’ve included a link to a video below as well which outlines many many aspects of FFA. You might find it helpful.
Good luck!
