Hair Breakage and Hair Growth in Central Centrifugal Cicatricial Alopecia (CCCA)
CCCA: How do I overcome my hair breakage?
I’ve selected this question below for this week’s question of the week. It allows us to the review some key concepts in the management of central centrifugal cicatricial alopecia (CCCA) and the importance of hair breakage in patients.
QUESTION
I recently was officially diagnosed with CCCA. I am a 35 year old black woman. I started having hair breakage on the vertex of my scalp since around June of last year. I stumbled across your papers, watched your seminars on youtube etc etc. and I had a strong suspicion that I had a diagnosis of central centrifugal cicatricial alopecia (CCCA).
I went to see the physician but by that time, my hair was growing back in that area (I had to wait several months to see a specialist) so the specialist did not think it was CCCA and diagnosed me with another hair condition called Trichorrhexis Nodosa as there were nodules on my hair shaft and I had a positive pull test.
Long story short, my hair seemed to be doing relatively well for awhile but around the end of March of this year, what seemed like overnight, I had hair breakage in my vertex again with the hair shaft super short. Basically I had a peach fuzz in that area. So I immediately called my dermatologist again and pushed for a biopsy. Three weeks later I was diagnosed with an inflammatory scarring alopecia, with the differential being CCCA.
This is what my biopsy said:
Microscopic Examination: There is concentric perifollicular fibrosis and the level of the isthmus, with associated patchy perifollicular lymphocytic inflammation. There are decreased sebaceous glands and focal interface dermatitis involving follicular epithelium. The features are of a lymphocytic inflammatory scarring alopecia, with the differential including lichen planopilaris and CCCA. Clinical correlation is recommended.
- Final Diagnosis SKIN BIOPSY SCALP: INFLAMMATORY SCARRING ALOPECIA"
So, now to my question.
I do not have any external scarring....as in I am not bald on any area of my scalp. I just have a small island maybe the size of a golf ball of short hair while the surrounding hair is significantly longer. At the end of March when I noticed the breakage, it was a peach fuzz. Since getting the biopsy and waiting on the results it has grown a little. It is now measured at a little less than 1.5 inches. So the hair in that area seems to be growing. However, will it grow continuously OR will it grow to a certain point and break off? I have internal follicular scarring at the level of the isthmus and my dermatologist told me that that is irreversible (though I want to explore the 10% metformin in Lidoderm that is hypothesized to reverse scarring).
So, assuming I had CCCA since last year, I am afraid that I will go through a cycle of hair growth to a couple inches and then breakage even if I am able to get the inflammation under control with the oral doxycycline and topical clobetasol that I was prescribed. I assume that the follicular fibrosis at the level of the isthmus has probably affected the formation or structure of the hair shaft and that's why some patients experience hair breakage early on in the disease? So, in your experience, have you seen continuous hair growth when CCCA is caught at the hair breakage stage or did it go through a cycle of grow and break?
Also, should I be taking clobetasol breaks? My dermatologist prescribed it once a day, every day indefinitely. Well, I suppose we will reassess when I see him again in 4 months but I remember reading on your site that you suggest steroid holidays every couple weeks. I use very little in that area daily as I am aware of, and afraid of any side effects.
ANSWER
This is a great question.
Hair breakage is very common in CCCA. In fact, hair breakage can be one of the very first clues that a patient has to the disease process. Hair breakage can happen prior to hair loss and prior to the appearance of ‘patches.’ You may wish to review a previous article I wrote:
Hair Breakage in Black Women: Not to Be OverLooked!
It’s true that “trichorrhexis nodosa” is associated with the hair breakage as you write - but the reason the hair is breaking in these situations is partly due to the underlying scarring alopecia. Heat and chemicals and hair styling might still have a role in some so that needs to be investigated in your case too. You and your dermatologists can review that.
The pattern that you describe of these short hairs that don’t seem to grow very long is very typical of CCCA. Usually these areas on the scalp are about the size of a tennis ball, although sometimes the area is bigger and sometimes smaller.
Hair breakage is common in CCCA and may appear as small patches about 2- 6 cm in diameter that simply fail to grow longer. Proper treatment of the CCCA reduces the inflammation under the scalp and sometimes helps the hairs to elongate and areas to fill in more normally.
This hair breakage issue is so important to recognize because it can be a sign of very early CCCA (or what I term subclinical CCCA).
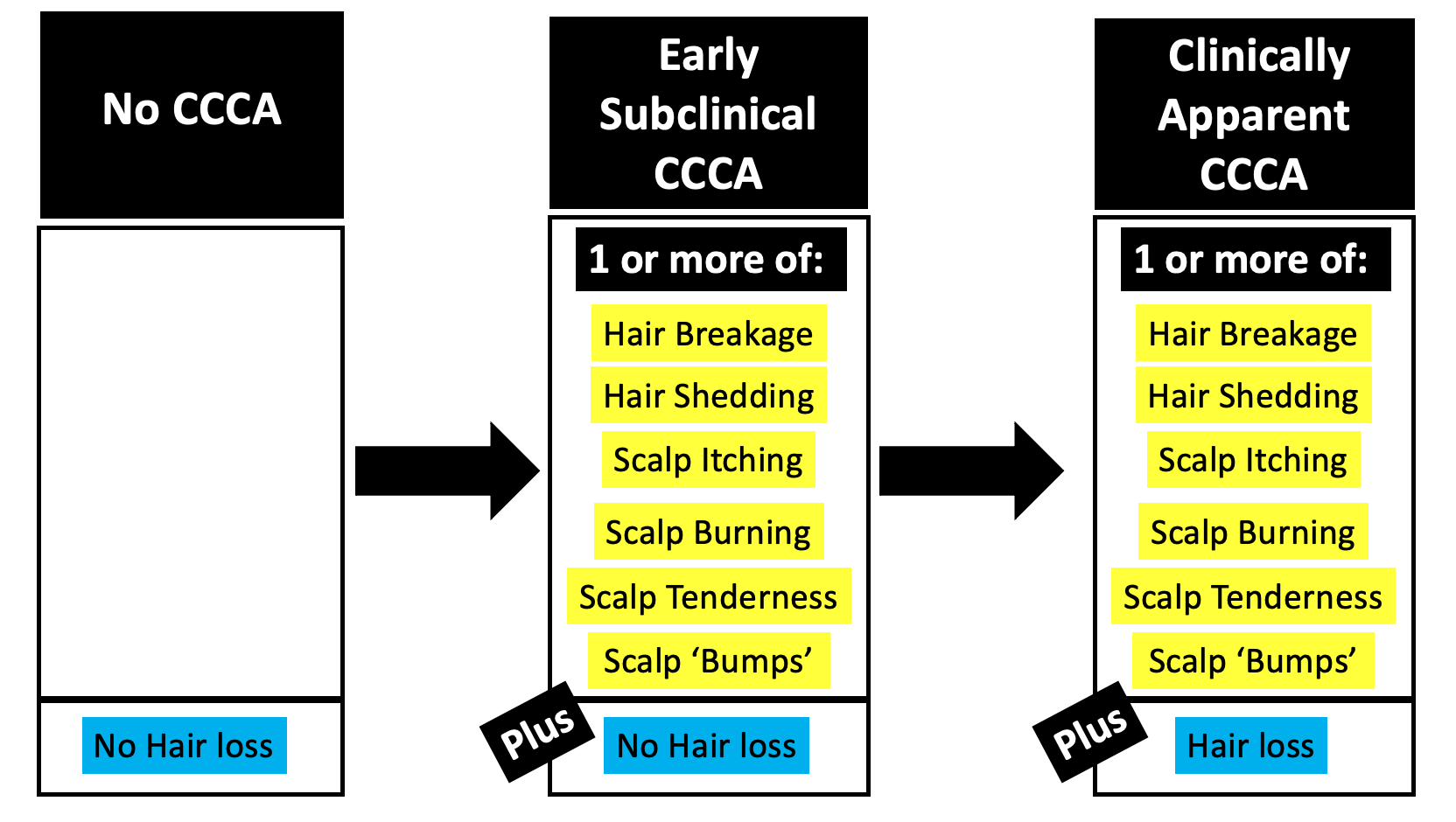
Will my hair grow longer?
These areas of short hair might grow longer - yes! It’s possible that’s for sure. However, the overall chances this area will regrow is higher if you choose to aggressively treat your scarring alopecia than if you choose to less aggressively treat your scarring alopecia. By “aggressive treatment”, I mean the use of a plan that really works to chase away inflammation. This plan might include periodic topical steroids with steroid injections and oral doxycycline. You and your doctors can decide what is right for you and if you have any specific contraindications to these medications (ie reasons why you should not use). Topical 10 % metformin is an option too but no it’s not a “first line” treatment. It is a newer treatment and it’s not clear how many it helps. Maybe someday it will be first line treatment, but it’s not right now. Topical metformin does not reverse scarring, that would not be correct. Nothing reverses scarring - that’s permanent. However, topical metformin most certainly can help with stopping inflammation and getting hairs to sprout back up. There is a big difference between helping with hair growth and reversing scarring. Many treatments for early staged scarring alopecia can get hairs growing and help the patient achieve improved density. But that’s not because it reverses scarring.
To review the treatments for CCCA, you might wish to review the prior article but I’ll go into it a bit more here to review.
It could be that topical steroids like clobetasol alone (as the sole treatment) might be sufficient to treat CCCA but for many women with CCCA, clobetasol alone is not enough to stop the disease. An aggressive approach might involve use of topical clobetasol with periodic steroid injections and a 3-6 month course of oral doxycycline. I am also a big fan of topical tacrolimus ointment as well in treating CCCA and it can be used with the clobetasol. How exactly these are used depends on the patient and her story and how much inflammation seems to be present. Treatment might initially involve daily clobetasol in the morning and tacroliumus in the evening or clobetasol three times weekly (Monday, Wednesday and Friday) and then Tacrolimus the other days. This is always re-evaluated every 3-5 months. No treatment is forever, except perhaps minoxidil if the patient also has a diagnosis of androgenetic alopecia.
I’m all very much a big fan of reducing heat and chemical as much as possible for at least 6 months. I know it’s not always possible but it does seem to help a great deal during this period where the hair is really weak. Your hair will be better able to tolerate heat and chemicals in the near future if we can get rid of the inflammation.
The ‘gold medal’ or first line treatments for CCCA are shown below together with second line (silver medalist) and third line treatments (bronze medalist):

You can see from the list above that 10 % metformin is certainly an option, but jumping on board with this as the first step would not be considered “first line”. There are only a small number of patient around the world treated with topical metformin so if that’s the route you want to take that’s fine. But know ahead of time that you are going at this without the backup of thousands upon thousands who have used the other first line treatments. It still could be a good option.
It may take 3-5 months to see changes but the patient often sees less breakage, less itching, less tenderness and this is followed by some degree of improvement. Early stages of CCCA are more likely to have some degree of improvement in terms of a bit of hair regrowth. Late stages usually do not.
I do feel that periodic breaks in using steroids are needed. I like my own patients to initially treat as aggressively as they are comfortable with. This means topical steroids daily for 4-6 weeks and then a 2-3 week holiday whereby no topical steroid are applied. This ‘holiday period’ is a great time for applying tacrolimus ointment as tacrolimus does not thin the skin and has very little in the way of absorption. After the two week clobetasol drug holiday is over, I might advise the patient to do another 4-6 weeks. However, if things are going well, we’ll often drop down to using clobetasol 3-4 days per week (and possibly use the Tacrolimus on some of the other days). So, to answer your question, use of clobetasol is not lifelong for patients with CCCA. Clobetasol is used until the point in time that we feel we don’t need daily treatment any more because of how good the scalp looks or feels or how well things are growing. But for those who need it, I have no issues with using clobetasol longer term provided we have some “steroid holiday” periods mixed in there.
It’s okay to be afraid of side effects, but periodic topical clobetasol, steroid injections, tacrolimus, and topical metformin are very well tolerated for the vast majority. Even doxycycline is well tolerated for most, although you’ll want to be comfortable with all the side effects of doxycycline if you go down that route.
All patients with CCCA need blood tests for CBC, TSH (thyroid studies), ferritin (iron), and 25 hyroxyvitamin D, glucose and hemoglobin A1c. If any of these are abnormal, they need to be addressed.
I hope this helps. If you treat the inflammation and limit injury to hairs for the next 6 months, you can break this hair breakage cycle.
Thank you again for the question.
Reference
Callender V et al Hair breakage as a presenting sign of early or occult central centrifugal cicatricial alopecia: clinicopathologic findings in 9 patients. Arch Dermatol. 2012 Sep;148(9):1047-52.