Oral Minoxidil - Can it cause rapid fluid retention?
Fluid Retention with Oral minoxidil
I’ve selected this question below for this week’s question of the week. It allows us to review some concepts related to the early onset of fluid retention with oral minoxidil treatment.
Question
Hi Dr Donovan,
I have started oral minoxidil for treating hair loss just 5 days ago and I now feel my face is puffier. I know that fluid retention can be a side effect but I have read that most people develop swelling around month 3. Do you think I could just be imagining it? Is swelling like this at day 5 even possible?
Answer
Thanks for the great question. There’s a few key things to be aware of here. First, the three month time point is the latest point at which most people will have experienced swelling it it is going to occur. In other words, if swelling and fluid retention has not occurred by month 3, there is a very high likelihood it will not occur. That’s why we advise patients to wait three months before making dose adjustments.
But the key fact not to miss is that humans differ in their responses to medications just like they differ in how their disease presents. For example, a very very low proportion of patients will start getting fluid retention around month 4, 5 or 6. It’s a low proportion - but nevertheless it’s real.
Similarly, a very low proportion of patients will develop fluid retention by month 1 and and even lower proportion will already have fluid retention by week 2-4.
The key point here is that the timing of fluid retention differs for everyone! For the vast majority - fluid retention if it is going to occur is starting to become an issue around month 2-3. But some are sooner than this and some are later.
Conclusion
It’s not impossible for a very small proportion of patients to have early onset fluid retention. It’s quite rare to have it by day 5 - but not absolutely impossible.
How best to proceed is handled on a case by case basis. So you and your doctor will want to sit down and review all this.
Some patients decide to stop for 2 weeks and then proceed with a plan that uses oral minoxidil at a lower dose. Some proceed with the same oral minoxidil dose and add a diuretic (torsaemide etc). In my professional opinion, there is a big difference between a patient scenario where a patient comes to see me and we ALREADY KNOW that minoxidil caused swelling and fluid retention and the scenario here where it is not yet clear.
My own advice is not to be on doses of oral minoxidil that cause fluid retention if possible. But we’ll go into that in a moment.
I would advise my own patients with similar stories to consider the following steps. (Whether this is a good idea for you should simply be confirmed with your own doctors).
1) the patient should weigh himself or herself today
2) the patient should take photos of his or her face today
3) the patient should stop minoxidil today
4) the patient should weigh himself or herself daily for the next 10 days and take photos daily for the next 10 days
5) the patient make consider restarting oral minoxidil in 10 days at a much lower dose than prior (assuming everything ultimately returned back to normal)
6) the patient should weigh himself or herself every day and take photos of the face every day for 2 weeks and then every 3 days for 2 weeks and then every 5 days for 2 months.
7) The dose can be increased at the three month mark if weight is stable and there is no observed puffiness, or fluid retention in the face or feet or weight gain
8) On the new dose, and every dose increase, the patient should again weigh himself or herself every day and take photos of the face every day for 2 weeks and then every 3 days for 2 weeks and then every 5 days for 2 months.
Together, these recordings on body weight and these photos will be helpful to assess if swelling truly is occurring. It’s takes only a few seconds to weigh oneself and only a few seconds to snap a photo. These two peices of information will be helpful for you and your doctors to determine if truly you are sensitive to the fluid retaining effects of minoxidil.
The timing of how often to take photos and the timing of how often to obtain a body weight depends on the possible speed of real or perceived fluid retention.
The following example would be in keeping with a minoxidil fluid retaining effect
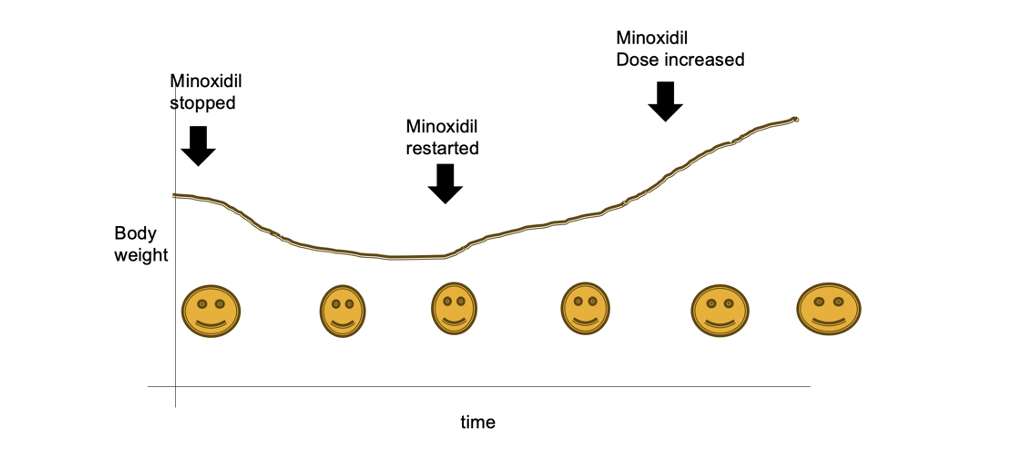
Changes in body weight and facial puffiness in a patient who is having a side effect of fluid retention from low dose oral minoxidil
Considerations for the Patient Already Using Oral minoxidil for many Months and now has Fluid Retention
The scenario above (i.e. the question of the week) pertained to a situation where the patient has JUST STARTED ORAL MINOXIDIL is not sure if minoxidil caused swelling. As reviewed above, my advice there is generally to get some good body weights by stepping on the scale, take some really good photos and then stop the dose for a while and then restart - again with lots of photos and lots of body weight measurements.
Now let’s look at a different scenario. What do we do when a patient has already been on oral minoxidil for some time? Consider the case of a 43 year old female patient who is referred to me regarding management of oral minoxidil side effects. She is ecstatic at her improvement on oral minoxidil. She was started 2.5 mg LDOM by a practitioner and now has considerable ankle swelling.
The options to consider here depend on the degree of fluid retention and the severity. If there is any amount of shortness of breath or marked body swelling or chest pain or dizziness, we have no choice by to stop the minoxidil and seek expert consultation. This may be from the emergency department or from a cardiologist. When patient’s present with swelling we need to ask ourselves “Where exactly could the swelling be?” If you are not willing to consider the possibility of fluid in the lungs, or accumulating around the heart or accumulating in the body, you are going to miss cases of pericardial effusions, pleural effusions and widespead anasarca. If you don’t know the basics of pericardial effusions, pleural effusions and anasarca, some might even say you probably should not be even prescribing oral minoxidil. Fortunately, these are extremely rare side effects - but yes, they do occur.
Below is a summary of a nice report from Dr Dlova and colleagues that reminds us all of the need to be humble when using LDOM
Now, let’s consider the more common scenario where the patient has swelling in the feet but there is no worries about cardiovascular or hemodynamic instability. The patient does not seem to have problems with breathing, chest pain, shortness of breath. There is no reason to suspect a pericardial effusion and no reason to suspect a pleural effusion.
The options here include such options as
1) reduce the dose of oral minoxidil to 1.25 mg or 1.875 mg and see what happens with fluid over time. There likely will be some hair loss with a dose reduction of LDOM.
2) reduce the dose of oral minoxidil to 1.25 mg or 1.875 mg and add spironolactone 50-100 mg once daily if there are no contraindications and the patient accepts the potential side effects. One would then see what happens with fluid over time. There may or may not be hair loss depending on how much the spironolactone can compensate.
3) reduce the dose of oral minoxidil to 1.25 mg or 1.875 mg and add spironolactone 50-100 mg and topical minoxidil if there are no contraindications and the patient accepts the potential side effects. One would then see what happens with fluid over time. There may or may not be hair loss depending on how much the spironolactone and topical minoxidil can compensate. This is an aggressive plan but reduces the likelihood of hair loss
4) reduce the dose of oral minoxidil to 1.25 mg or 1.875 mg and start topical 5% minoxidil if he patient accepts the potential side effects and see what happens with fluid over time. There may or may not be hair loss depending on how much the extra topical minoxidil can compensate
5) continue the 2.5 mg oral minoxidil and start a diuretic if there are no contraindications and the patient accepts the potential side effects.. This might include torsamide in countries where it is available or hydrochlorothiazide or furosemide. This is not without risk of side effects from the diuretic itself and diuretic side effects needs to be thoroughly reviewed with patients.
6) continue 2.5 mg oral minoxidil and severely salt restrict. The fluid retention with oral minoxidil does seem to be dependent on sodium intake (at least a bit). Many people who are high salt users notice marked improvements once they reduce their salt intake.