Childhood and Adolescent Onset Androgenetic Alopecia
What are the Features of Pediatric Male and Female Pattern Hair Loss?
Androgenetic alopecia (“balding”) can occur in both children, adolescents and adults. Of course, it comes as no surprise that this diagnosis is quite rare in children and still quite uncommon in adolescents. About 0.5 % to as high as 2 % of high school students are thought to have androgenetic alopecia. By the age of 50, about 50 % of males will have this condition and 20% of women. By the age of 85, about 85% of men will have AGA and 50 % of women. The onset of androgenetic alopecia in children and adolescents is a really important topic and one that we’ve covered before. (See “Chilldhood and Adolescent Onset Androgenetic Alopecia: Key Lessons”). I define childhood onset AGA as androgenetic alopecia occurring before puberty and adolescent onset AGA as androgenetic alopecia starting after the onset of puberty but before age 18. It’s not clear if early onset androgenetic alopecia is becoming more common or not but some believe that it probably is. The exact reasons why are not clear but environmental factors - including food products - as well as obesity may play a role.
The Özcan Study of 2022
Özcan from the Dept of Dermatology in Ankara Turkey set out to evaluate the demographics, medical and family histories, clinical and trichoscopic features, androgenic hormones, and metabolic syndrome risk factors in pediatric androgenetic alopecia. To do so, the author reviewed the medical records of 23 pediatric patients diagnosed with AGA between December 2015 and June 2020. These 23 patients included 12 females and 11 males with a mean age of 15.3. 16 patients had adolescent AGA (8 females and 8 males; mean age: 16.3) and 7 patients had childhood AGA (4 females and 3 males; mean age: 12.9)
Do patients with Pediatric AGA have a Family History of AGA?
A family history of patterned hair loss in a first-degree relative was not present in all patients. In fact, a family history occurred in only 9 (56.3%) of 16 patients with adolescent AGA (six males, three females). Six males had only their father, and two females had only their mother, and one female had both parents affected. None of the patients with childhood AGA reported a family history in the first-degree relatives.
What medical conditions do Patients with Pediatric AGA have?
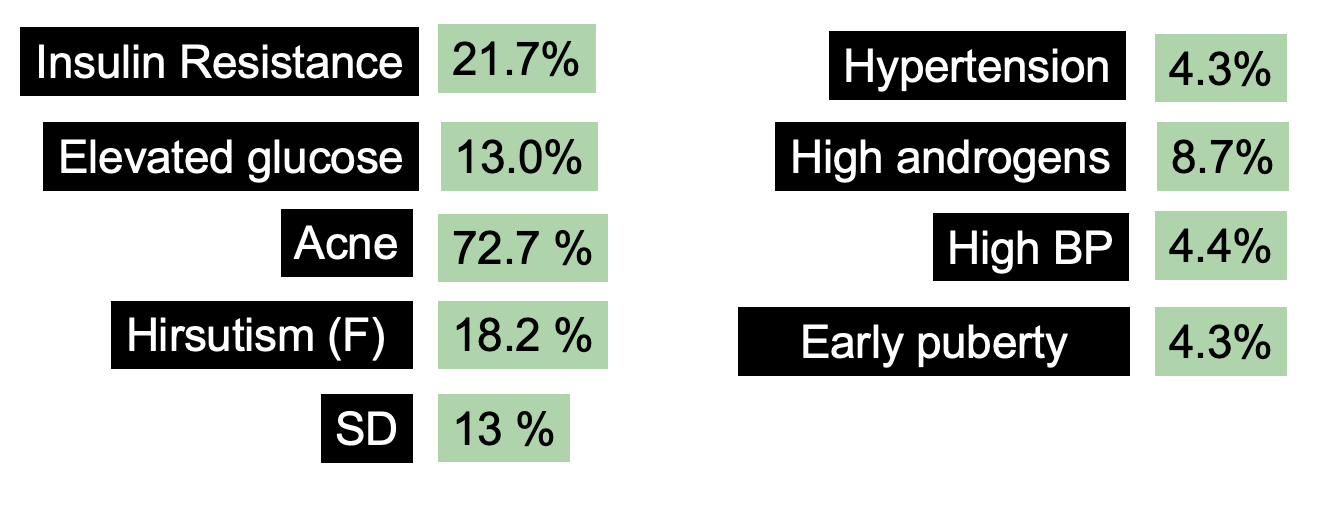
Two of 8 females with adolescent AGA had a previous history of insulin resistance, and one female with adolescent AGA reported a history of PCOS. One of the females with IR also had associated hypertension. Concurrent skin diseases were noted in 11 (47.8%) of 23 patients. Of those, eight patients (72.7%) (five males, three females) had acne and three patients (27.3%) (two females, one male) had seborrheic dermatitis. Hirsutism was noted in two females, one of whom also had seborrheic dermatitis. The patients’ sexual development and growth parameters were appropriate for their ages except for one female with early puberty, hirsutism, and seborrheic dermatitis. Fourteen patients (60.9%) with pediatric AGA (10 adolescents and four childhood AGA, eight females and six males) had at least one of the risk factors of MetS such as obesity, high blood pressure and insulin resistance.
Do patients with pediatric AGA have abnormal test results?
Insulin resistance was noted in 21.7% of patients and elevated fasting glucose was noted in 13 % of patients. Lipid abnormalities were found in 4.4 % of patients and elevated androgens were noted in 8.7 % of patients. 4.4 % of patients had elevated blood pressure.
What Patterns of Hair Loss and Thinning were Noted?
The most common hair loss pattern was diffuse thinning at the crown with preservation of the frontal hairline and this was observed in 10 (43.5%) of 23 patients with pediatric AGA. The next most common was a ‘‘Christmas tree’’ pattern in four (17.4%), bitemporal, frontoparietal, and vertex thinning in three (13%), diffuse thinning pronounced at the crown with bitemporal thinning in three (13%), bitemporal and vertex thinning in two (8.7%) patients, and diffuse thinning pronounced at the crown in one patient (4.4%).
Crown thinning was a common presentation in males and females. Six (54.5%) of 11 males had diffuse thinning at the crown with preservation of the frontal hairline. Among the females, the most frequent clinical presentations were diffuse thinning at the crown with preservation of the frontal hairline and ‘‘Christmas tree’’ pattern, each observed in four (33.3%) of 12 females
Conclusions
This is an interesting study. The study supports that notion that children and adolescents with AGA may have one or more risk factors for metabolic syndrome.
Contrary to the belief of many people, hyperandrogenism was not a common finding in this study. Furthermore, many patients did not have a strong family history of AGA. This is important to note as it is quite difficult sometimes for parents to understand how their child could have androgenetic alopecia when neither parent is affected.
Limitations to the study include its small size and lack of a control group. We can’t say that certain values or parameters are increased in children with AGA compared to children without AGA as this was not studied.
Listen to this study on Dr. Donovan’s Evidence Based Hair Podcast
REFERENCE
Özcan D. Pediatric androgenetic alopecia: a retrospective review of clinical characteristics, hormonal assays and metabolic syndrome risk factors in 23 patients An Bras Dermatol. 2022 Jan 12;S0365-0596(21)00308-1.
This article was written by Dr. Jeff Donovan, a Canadian and US board certified dermatologist specializing exclusively in hair loss.