Combining Treatments: Do Two Treatments Always Help More than One?
Combining Treatments for Hair Loss
We frequently need more than one treatment strategy to stop a hair loss condition or to get the hair growing in the way we want it to grow. But there is more to think about when we combine treatments than is sometimes considered.
There are countless examples of combinations of treatments that take place in the clinic every day:
I might recommend starting hydroxychloroquine to a patient with lichen planopilaris who is already using a topical steroid in hopes that their disease calms down even better.
I might recommend that a patient with alopecia areata who has been receiving monthly steroid injections also start topical minoxidil on the patches of hair loss
I might recommend that a patient with frontal fibrosing alopecia start isotretinoin in addition to the finasteride, hydroxychloroquine and steroid injections they are currently using.
Combining Treatments: Are they doubly effective ?
Most patients with hair loss want to gather as much information as possible as it pertains to their hair loss. For example, if patients learn that treatment A helps 30 % of patients and treatment B helps 50 % of patients, they want to know if using both treatments will help help 80% of patients? In a similar line of thinking, if treatment C is thought to regrow 10 % of the hair back and treatment D is proposed to grow back 25 % of the hair, will using both of these treatments help grow back 35 % of the hair?
These are wonderful questions and often the answers patients get are often quite vague. Let’s take a look at the effects of combining treatments. The main point is that many treatments for hair loss are slightly additive.
Evaluating Success of Treatment - The Treatment Outcome Scale
Before we start, let’s review together an arbitrary scale for evaluating the effective of treatment. Here’s the scale I’ve used for quite some time now:

What can happen when we combine two treatments?
OPTION 1: The combination of treatments is “slightly additive”
This is the most common scenario and the most easily confused. Consider Treatment A and Treatment B. Treatment A helps the given type of hair loss a bit (Let’s call it 2 plus per the scale above)) and Treatment B helps it a little bit as well (let’s call it 3 plus per the scale above). When treatments A and B are combined the result is 4 plus. The hope would be that combining the two we might get a 5 plus or maybe a 6 plus but it ends up now helping quite that much
The reality is the combination of the two is better than using either alone, but it’s not quite additive and using the two does not lead to any type of synergistic outcome that would be even better than predicted.
This is the most common scenario we see in treating hair loss. If treatment 1 helps a bit, the effect of adding treatment 2 is to see a a bit more help compared to using either treatment 1 alone or treatment 2 alone. The combination of two treatments does not often lead to massive improvements compared to what each is capable of doing alone. Sometimes of course we see no benefit at all of adding treatment 2.
In this example, consider the patient with lichen planopilaris who has been using topical clobetasol. This treatment has helped a bit and the patient’s redness and itchiness has certainly been reduced. Now consider what happens when we add oral doxycycline to the patient’s treatment plan. We’re hoping that the doxycycline takes the redness, itchiness and hair loss down a great deal more. sometimes what happens however, is that the disease activity gets reduce a bit more than we saw when the patient was only using clobetasol but not quite as much as we were hoping. IN others words the treatments are slightly additive but not fully additive.
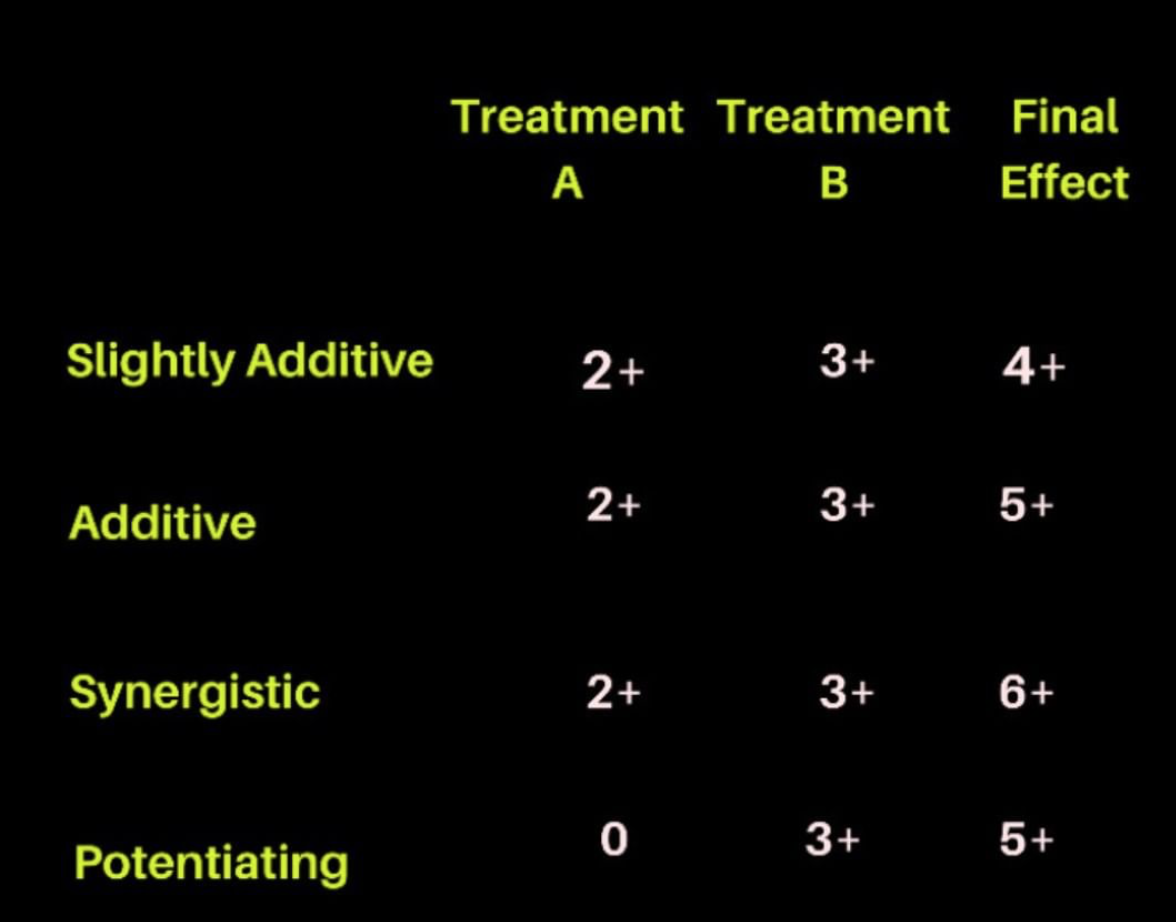
OPTION 2: The combination of treatments is “additive”
Sometimes, when we combine treatments we see additive effects. Treatment A helps 2 plus per the scale above and treatment B helps 3 plus and when we combine the two together, the patient gets a 5 plus. The result is better than we can achieve with either one alone. The outcome of using the treatment is not synergist because it does seem that treatment A relies on treatment B or vice versa. The two treatments just direct the hair follicle in the correct manner.
We sometimes see additive effects when treating hair loss - and when we do, it’s wonderful. For example, in the treatment of frontal fibrosing alopecia, combining finasteride and isotretinoin “sometimes” seems to have additive effects. Furthermore, from time to time when treating male androgenetic alopecia we see additive effects with minoxidil and finasteride. From time to time when treating lichen planopilaris (LPP), we see additive effects with a topical steroid and oral immunosuppressant. Of course, we don’t always see additive effects in these three examples by any means.
OPTION 3: The combination of treatments is “synergistic”
We don’t often often see treatment that are truly ‘synergistic.’ In a synergistic treatment plan, treatment A might helps 2 plus per the scale above and treatment B helps 3 plus and when we combine the two together, the patient gets a 6 plus. The result is better than we can achieve with either one alone and more than simply additive. In a synergistic effects, treatment A works better because treatment B is also being used (or vice versa). We do sometimes see synergistic responses with use of topical steroids and topical minoxidil in the treatment of alopecia areata. The topical steroid helps minoxidil absorption in some cases depending on the vehicle used.
OPTION 4: The combination of treatments involves “potentiating effects”
We don’t see potentiating effects all the often, but I’ll explain what this means and where we do see them. In a treatment plan involving so called potentiating effects, treatment B helps hair loss. Treatment A on the other hand actually does nothing on its own. However, when combined with treatment A, treatment B now works much better. For example, treatment B might helps 3 plus (per the scale above) but when combined with treatment A, treatment B now helps 5 plus. As mentioned above, treatment A on its own helps 0.
A good example is the effect of shaving the scalp in some males with folliculitis decalvans - a type of scarring alopecia. Shaving (treatment A) has no effect on the disease folliculitis decalvans itself. Shaving doesn’t help the disease and doesn’t worsen the disease. This is treatment A. However, when using a topical antibacterial agent or topical cleanser, sometimes shaving the scalp actually helps the topical treatments work better. The medications find their way into the scalp better when the scalp is shaved. There is literature and studies to back this up for any skeptics. But in this case, the act of shaving potentiates the effect of the standard topical treatments.
Conclusion
When we start a second treatment in a patient who is already using one treatment, there are several things that might be observed. It’s possible the new treatment provides no further benefit or it possible it provides a slight degree or even a large degree of improvement. We refer to these as additive effects. Sometimes that new treatment helps much more than would have been predicted from using the treatment all be itself (potentiating effects).
This article was written by Dr. Jeff Donovan, a Canadian and US board certified dermatologist specializing exclusively in hair loss.