Treating Androgenetic Alopecia in Males Adolescents vs Adults
How should my 16 year old son’s AGA be treated?
I’ve selected this question below for this week’s question of the week. It allows us to review some concepts regarding treatment of androgenetic alopecia in male teenagers and how this differs in adults.
Question
My son is 16 years old and it’s clear he has androgenetic alopecia. We have seen several dermatologists but we’re unclear as to how and when and what treatments should be started? What is your approach to treating androgenetic alopecia in a teenager … and how does this differ from how it is treated in an adult?
Answer
Thanks for the great question.
We’ll dive deeper into the question in one moment but there are a few principles that are important to state at the outset:
1) There are no FDA approved treatments for teenagers - so everything is ‘off label.’ That does not mean there are no treatments but it does mean there are no FDA approved treatments.
2) Treatment should be started earlier than later if the goal is to stop the hair loss.
3) We need to support the teenager’s psychological development. Don’t underestimate the harm that can be done by various misguided approaches. The focus is on the well-being of the patient not the hair. Screening for depression and anxiety is important for any age but especially this age.
4) Treatments are lifelong.
5) Minoxidil is at the top of the list. It may or may not ultimately prove to be helpful but step 1 is easy. Steps 2, 3 4, and 5 afterwards is where the real discussion and expertise comes into effect. Step 1 is easy.
6) Hair transplants are not an option until 23 years of age for the frontal area - and preferably 25-26. The crown should not be transplanted until 30-35. If you get the opinion that hair transplants are a good idea in young patients 18-22 years of age, go get 5 more opinions from surgeons that have practiced more than 20 years.
7) A basic “work up” is important including fasting blood sugar, fasting cholesterol, TSH, ferritin, free and total testosterone, DHEAS, AM cortisol, prolactin and 17 hydroxyprogesterone. Consideration can be given to estradiol, LH and FSH in female patients. Where possible, blood tests for females should be performed on day 3-5 of the menstrual cycle.
8) Blood pressure, weight and height should be measured.
A Closer Look at Childhood and Adolescent Onset AGA
Childhood onset AGA and adolescent onset AGA (AO-AGA) are special subtypes of early onset AGA. Childhood onset AGA is a term that refers to AGA starting before puberty and adolescent onset AGA is a term to refer to androgenetic alopecia starting after puberty but prior to age 18. The exact prevalence is not clear but it’s likely that 0.5 to 2 % of high school students shown signs of androgenetic alopecia. A 2010 survey by Trancik et al of 84 physicians who provided data on 448 adolescents with early onset androgenetic alopecia ( 341 boys and 107 girls), hair loss began between ages 7 and 17 years. The mean age at onset of 14.8 years in boys and 13.8 years in girls. Your son’s onset is early for male balding but not early for what we see which those who develop adolescent onset AGA.
The general features of adolescent AGA are similar to adult onset AGA, namely the ‘miniaturization’ of hair follicles. The frontal hairline is less commonly affected in the early stages compared to male adults with AGA.
Family History
A family history of thinning may be present in some but not all cases. In my opinion, one should not be all that confused if the child or teen in front of the doctor has AGA but the parents do not. It’s difficult for parents to accept but a good proportion (ie 25-40%) of males with early onset AGA don’t have a strong family history. It’s a bit more uncommon for an adult to have AGA without some kind of family history. Still not impossible but more uncommonly encountered compared to children and adolescents with AGA.
Systemic Issues for Patients with Early Onset AGA
Most children and teens with AGA are healthy. However, one needs to be on the lookout for several uncommon conditions. Missing a condition is not good for any age, but missing a condition in a child leads to a lot more years of harm than for an adult. A practitioner MUST be comfortable answering these questions below in any child or teen with AGA. If they don’t know how to answer the question, they MUST refer to someone who does.
QUESTIONS FOR THE PRACTITIONER TO ANSWER REGARDING MALE PATIENTS WITH ONSET OF AGA BEFORE 18 YEARS:
1) Does the child or teen with AGA have high blood pressure?
2) Does the child or teen with AGA have high fasting glucose?
3) Does the child or teen with AGA have insulin resistance?
4) Does the child or teen with AGA have obesity?
5) Does the child or teen with AGA have elevated cholesterol/lipids?
6) Does the child or teen with AGA have congenital adrenal hyperplasia?
7) Does the child or teen with AGA have elevated androgens?
8) Does the patient with AGA have early onset of puberty?
9) Does the patient with AGA have acne?
10) Are there any other scalp conditions present (seborrheic dermatitis, AA, TE?)
QUESTIONS FOR THE PRACTITIONER TO FOR FEMALE PATIENTS WITH ONSET OF AGA BEFORE 18 YEARS:
1) Does the child or teen with AGA have high blood pressure?
2) Does the child or teen with AGA have high fasting glucose?
3) Does the child or teen with AGA have insulin resistance?
4) Does the child or teen with AGA have obesity?
5) Does the child or teen with AGA have elevated cholesterol/lipids?
6) Does the child or teen with AGA have congenital adrenal hyperplasia?
7) Does the patient with AGA have PCOS?
8) Does the patient with AGA have hirsutism?
9) Does the patient with AGA have acne?
10) Does the patient with AGA have early onset of puberty?
11) Does the child or teen with AGA have elevated androgens?
12) Are there any other scalp conditions present (seborrheic dermatitis, AA, TE?)
Questions Help Screen Underlying Issues
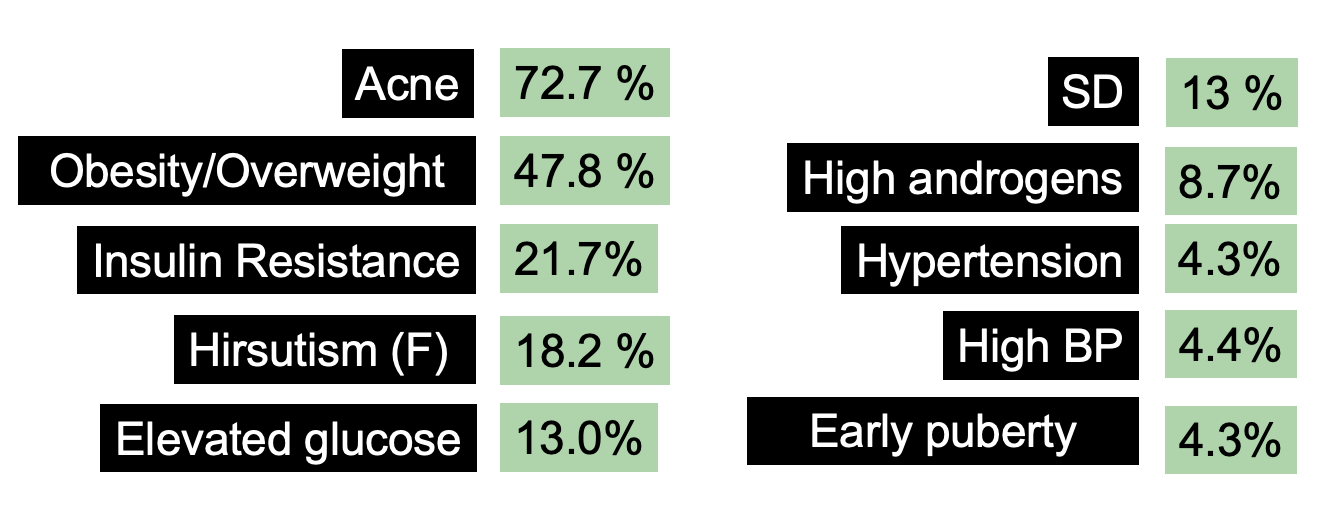
I won’t go into all the reasons why these questions need to be answered as that will take a bit of time. The main point is that the vast majority of children and adolescents with AGA are fairly healthy but 50-60% have risk factors for metabolic syndrome (like obesity, insulin resistance, high blood pressure and high blood sugars). One needs to look for these and address them fully. A very small proportion of children and adolescents with AGA have elevated androgens, high blood pressure, high cholesterol — but it’s well under 10 %. Nevertheless, these issues can be silent and so need to be explored.
A recent study by Ozcan showed that insulin resistance was the most common issue in pediatric onset AGA and a large proportion ( around 60%) had at least one risk factor for metabolic syndrome.
One needs to be comfortable ruling out various endocrine issues especially congenital adrenal hyperplasia and PCOS. Gonzalez et al showed that 1 out of 25 males adolescents with early onset balding had late onset CAH. A high proportion of females with early onset AGA have PCOS. In fact, elevated androgens were identified in 6 of 16 girls (38 %) with early onset hair loss and a diagnosis of PCOS was felt to be likely in all 6 patients.
Now back to your question ! What treatment?
Minoxidil is Likely to Be Step 1.
The treatments for adolescent AGA in males is slightly different than for adults given that we place greater emphasis on the use of minoxidil and less emphasis on the use of anti androgens in those under 18. To date, there are no formally “FDA approved” treatments for those under 18 years. That is not to say that there are no treatments simply that no company has submitted data to Health Canada or the FDA to have their product specifically approved for adolescents
In the absence of an underlying endocrine issue, minoxidil remains the first line option for treating adolescent AGA. In 2001, Trancik et al reported finings of 448 adolescents with androgenetic alopecia who were treated with minoxidil for 18 months. For the 341 males using minoxidil, 55 % had improvement in hair density and 41 % had a slowing of thinning. For the 107 females using minoxidil, 51 % had improvement in hair density and 44 % had a slowing of thinning. In a second 2010 study by Gonzalez et al, 4 of 6 girls (67%) and 18 of 23 boys (78%) who were treated with 5% minoxidil for more than 6 months had a stabilization of their hair loss.
Minoxidil appears to be safe in those under 18. In fact, an open-label investigation of 13 boys, aged 13 to 17 years (mean age, 15.9 years), with early male balding confirmed this safety. Participants applied 1 mL of minoxidil topical solution 5% to the area of thinning hair every morning and evening for one week minoxidil topical solution did not alter pulse rate, blood pressure, or other vital signs.
2) After minoxidil, a Variety of Treatment Options Exist
Other options for treating early balding include low level laser and I typically will add that early on in the course of treatment after topical minoxidil. Oral minoxidil can be considered too. The use of finasteride in males has not been formally studied under 18 and is not typically started until 17-18 year of age. I generally start topical finasteride well ahead of oral finasteride in young males if we decide that this is the right way to proceed. Spironolactone and oral contraceptives may be considered in some females especially if PCOS or CAH is an associated diagnosis.
I don’t think PRP in children and adolescents is practical. I would discourage it. The safety of topical minoxidil is very good and so is low level laser. These need to be explored first. PRP is traumatic, and I think this is to be avoided in children and adolescents unless truly needed.
other conditions like coexistent telogen effluvium or seborrheic dermatitis need to be treated. Some adolescent females have low ferritin levels and this needs to be addressed to optimize hair cycling. Some patients have seborrheic dermatitis and anti-dandruff shampoos are needed.
Full Care for the Child or Adolescent with AGA: What other steps are needed?
We do not yet have screening guidelines in the world for how best to monitor males and females with childhood onset AGA and adolescent onset AGA. We know confidently that males and females with early onset androgenetic alopecia have an increased risk of developing metabolic syndrome and cardiovascular disease later in life. I feel strongly that our medical community has neglected this issue but nevertheless we have guidelines in our clinic that we feel are appropriate first steps. In our clinic, we recommend the following:
1. Encouragement of healthy eating and diets rich in antioxidant rich fruits and vegetables.
2. Encouragement of active lifestyles with 300 minutes of physical exercise weekly.
3. Smoking cessation strategies for all smokers and guidance to not begin smoking.
4. Blood pressure measurements at baseline and then yearly by the pediatrician or family physician. Treatment of hypertension with lifestyle and pharmacological means as recommended by current evidence based guidelines
5. Cholesterol levels at baseline and then every 3-5 years. Aggressive treatment of abnormal cholesterol level according to current evidence based guidelines.
6. Fasting glucose insulin and hemoglobin A1c levels at baseline and every 3-5 years.
7. Weight and height measurements yearly and evidence based weight reduction strategies if weight rises into the overweight or obese ranges
Conclusions and Summary
I appreciated the great question. There are many similarities between adults and adolescents. In children and adolescents we have the radar finely tuned to identify any underlying abnormalities. Fortunately, most children are healthy.
Adolescent onset AGA is not common but carries significant psychological impact on teenagers. First and foremost, we need to make sure the psychological well being of the patient is placed front and center. Most parents are incredible but some add to their children’s stress. I can say that because I’ve cared for very large numbers of patients. That’s a sensitive subject but one needs to be aware that some parents impede the healthy development and adjustment to hair loss. We need to keep a close eye on this. Support, compassion, listening and understanding and and focus on the positive are the key things to promote. Depression and anxiety are real.
Getting a proper diagnosis is essential followed by initiation of treatment. In most cases, minoxidil will be an important first line consideration. Other options may be possible too. For males and females, it’s important to exclude an underlying endocrine issue.
References
Gonzalez ME et al. Br J Dermatol 2010.
Trancik RJ, et al Clinician survey evaluating minoxidil topical solution in the treatment of androgenetic alopecia in patients under 18 years of age. Poster presented at: 3rd Intercontinental Meeting of the Hair Research Societies; June 13-15, 2001; Tokyo, Japan. P129.
Özcan D. Pediatric androgenetic alopecia: a retrospective review of clinical characteristics, hormonal assays and metabolic syndrome risk factors in 23 patients An Bras Dermatol. 2022 Jan 12;
Trancik RJ et al. Investigation of the systemic bioavailability of 5% minoxidil topical solution in young males with early androgenetic alopecia. Poster presented at: 3rd Intercontinental Meeting of the Hair Research Societies; June 13-15, 2001; Tokyo, Japan. P126.