Treatment of Beard Hair Loss in Male Frontal Fibrosing Alopecia (FFA)
Beard Hair Loss in Males with FFA
I’ve selected this question below for this week’s question of the week. It allows us to review treatments for beard hair loss in males with FFA.
Question
I was diagnosed with LPP three months ago. My beard and hair are falling. Also persistent redness is in the beard area. My dermatologist started a steroid (1 month course) and 200 mg hydroxychloroquine treatment. We’re almost in the third month, but I continue see how my beard hairs are falling. Do you think is better to go with Methotrexate instead of keep trying with Hydroxychloroquine? I do not want to lose all my beard hair.
I am male, 34 yo, with itching and redness, hair shedding. I’m on hydroxychloroquine with oral Minoxidil and isotretinoin, healthy man, I’m in the third month of treatment, the hair starts to falling in March and begins in my beard, I lost some of the beard and hair.
Answer
Thanks for this really important question. In case you have not had a chance to review it yet, be sure to review the article on male frontal fibrosing alopecia that I wrote a few weeks ago. It summarizes all the studies on FFA in males published so far. As you’ll see in that article, there is alot of information summarizing the features of male FFA, but few that actually review treatment for FFA in males and fewer yet that specifically focus on the treatment of beard FFA.
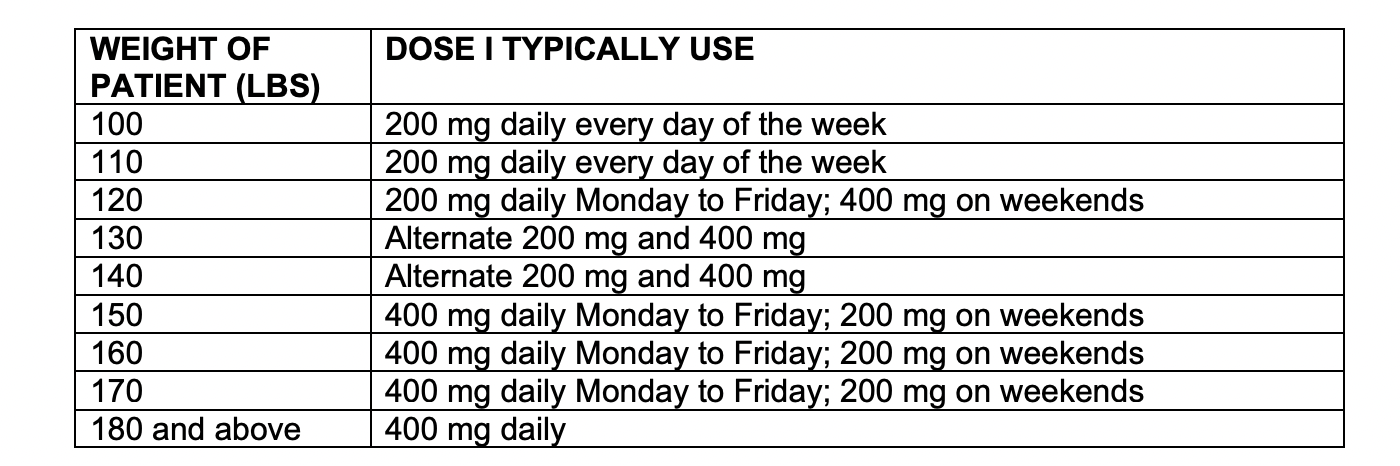
It sounds like you are on a really good starting plan. My feeling is generally that I would not abandon a ‘potentially’ good treatment too soon. There is some evidence from medical studies that hydroxychloroquine can help males with FFA. I think that you and your dermatologist may want to make sure you are on an appropriate dose of hydroxychloroquine. Depending on your weight, it might be possible to go up on the dose. The following table is a guide:
It may be possible at this stage to add some very safe treatments to ‘help out’ the hydroxychloroquine and the isotretinoin. I can’t say what is right for you specifically as I don’t know all your information but this might include a mild topical steroid once or twice weekly and the use of a non-steroid like topical pimecroliumus, topical tacrolimus or having a compounding pharmacist make up topical tofacitinib (if possible to do so in your country). I do support using the non steroid quite often because the non steroid does not cause atrophy and generally won’t cause steroid telangiectasias (redness from dilated blood vessels). The beard area in FFA can often be red so we don’t want to over do the steroid effect.
I also advise many of my own patients to start oral cetirizine as this has a pretty good safety profile overall and may provide benefit. 10-20 mg is often used.
Oral minoxidil, isotretinoin and hydroxychloroquine are part of a really solid plan. These other options (cetirizine, topical steroid and topical non steroids) may help. As far as the scalp goes, I am a big fan of getting my own patients on topical or oral finasteride or dutasteride because of how well it helps the scalp. As far as the beard goes, we don’t have any evidence finasteride or dutasteride actually helps the beard in FFA but we also don’t have any evidence that it does not. It could be that finasteride and dutasteride are not only antiandrogenic - but antifibrotic or antinflammatory in some other way.
I would encourage you to take photos of the scalp and beard and eyebrows every 4 weeks. If you have not already, I would encourage you to take a set of photographs today. This will be really helpful as this is what is going to guide you and your doctors about what to do next.
There are two choices if the plan discussed above still does not seem to be working. The first would be to stop the isotretinoin and add oral doxycycline. Doxycycline can be used with hydroxychloroquine but doxycycline can not be used with isotretinoin due to an interaction between the two drugs. This step might be considered before methotrexate but there is nothing really wrong with going to methotrexate immediately next. One of the reasons I often recommend doxycycline over methotrexate to my own patients is because it is safer overall. I often combine hydroxychloroquine with doxycycline (100 mg once to twice daily) and cetrizine (10 mg to 20 mg daily) and add on low dose naltrexone (3 mg nightly) if needed. Topical fluocinonide “gel” is used on the beard once to twice weekly and topical tofacitinib or topical tacrolimus is used 3-5 times weekly on the beard.
In refractory cases, I start methotrexate or cyclosporine or apremilast.
Thanks again for the great question. I do think you are on a really solid plan and you’ve got a good plan for second steps if this does not work. We still don’t have great research studies to guide us as to exactly what to do next but I hope these suggestions are helpful for you.
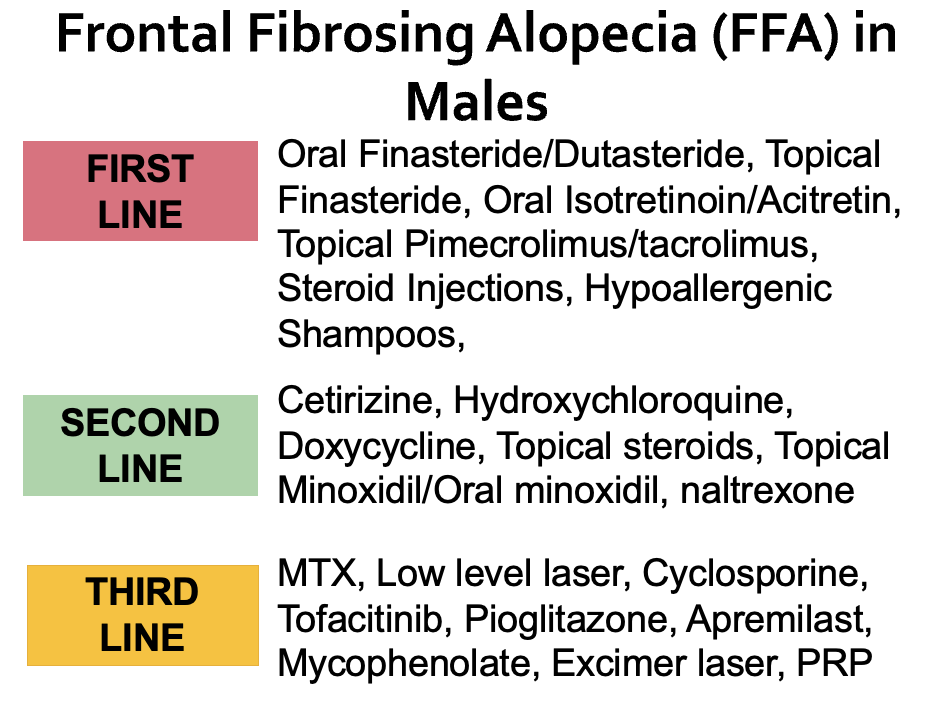
Here is a list of first, second line and third line treatment (in my opinion) for FFA. As I mentioned above, how best to treat beard FFA is not clear. But this is a general approach.