What is normal shedding? A Closer Look at SEVEN Key Points.
Is my shedding normal?
I’ve selected this question below for this week’s question of the week. It allows us to discuss some of the finer aspects of shedding and why 7 main considerations matter when it comes to evaluating shedding:
Here is the question….
QUESTION
I have been keeping track of my shed hairs as closely as possible for 70 days. My 30 day moving average is a steady 40 hairs per day and my 5 day moving average ranges from 38 to 42 or so. However, my daily shed is unstable and can range from 20 to 60 with periodic days of 70. The 60 and especially the 70 hairs a day concern me. Is it normal for your daily shed to fluctuate this much even though your averages are stable?
I am a 37 year old female.
ANSWER
Thanks for the question. There’s a lot to discuss with your question, so let’s get to it!
Before we go further, I’d like to point out that the ideal way to diagnose hair loss is using what I termed the ”Diagnostic S.E.T.” I refer to these as the diagnostic “set” because theses 3 aspects all go together. These 3 items include:
1) the patient’s Story
2) the findings uncovered during the process of the scalp examination and
3) the results of relevant blood tests.
The first letter of each of the three words 1) story, 2) examination and 3) tests spell out the word “S.E.T.” - again a helpful reminder of how the information obtained from reviewing each of these 3 aspects helps solidify a proper diagnosis.
I’d like to know a lot more about this story ideally but of course the magic of the “question of the week” is that I tackle questions with limited information. We’ll review 7 key questions in a moment. Other questions may also be helpful. I’d like to know what blood tests were done in your case and what the results were. I’d like to know if your menstrual cycles are now regular. I’d like to know if the person asking the question has any medical issues or takes any medications. I’d like to know about stress levels? I’d like to know her family history of hair loss. I’d like to know if the patient has lost any brows or lashes. I’d like to know if her weight has been stable? I’d like to know if the density is the same as 6 months ago or actually worse? I’d like to know if the patient has any headaches, joint pains, skin rashes, dry eyes, dry mouth, thirst, abdominal pain, fatigue, changes in libido, or ulcers the mouth. All these things matter in fully answering these questions.
With that behind us, let's return to our question of the week again!
With the information given in the question submitted, one can not get to the diagnosis. That requires a more full review of your story from A to Z …. and it requires examination of the scalp or at least photos. But let’s explore how we get to the answer.
It’s possible that the shedding here is just a variation of normal. We need to keep that in mind. Many people with your story have normal shedding. If you feel your hair density at age 37 is the same as age 25 and if you feel that your shedding rates are pretty similar now to what they were like at age 25, then it’s likely this is a variation of normal ! If not, then more work is needed for you and your doctors to get to the answer as to whether your shedding is normal or not. Hair loss conditions such as androgenetic alopecia and telogen effluvium are very much a possibility too. Conditions such as chronic telogen effluvium, alopecia areata incognito and scarring alopecia are possible with anyone with the story given in your submission, but the chances of these are pretty low overall. Statistically speaking, most likely a person with your story has either a normal variation or has androgenetic alopecia or has telogen effluvium or has BOTH androgenetic alopecia and telogen effluvium. An astute hair specialist can help you solve the mystery once they gather from you more information, examine your scalp and review some key blood tests with you.
If you really want to understand more about your shedding and what it means, you may wish to review things in detail with your dermatologist. He or she might order a 5 day modified hair wash test. This test takes time and patience to perform yourself at home, but it gives a wonderful amount of information. You can read more about it in the link above. A scalp biopsy is not advised in most cases of someone asking about shedding because the diagnosis can be determined by using the principles discussed above (the SET principles).
As well, as you think about your own shedding, you and your hair specialists can refer to the helpful table below.
Let’s take a look at this table and let’s review some key things we can learn from it.
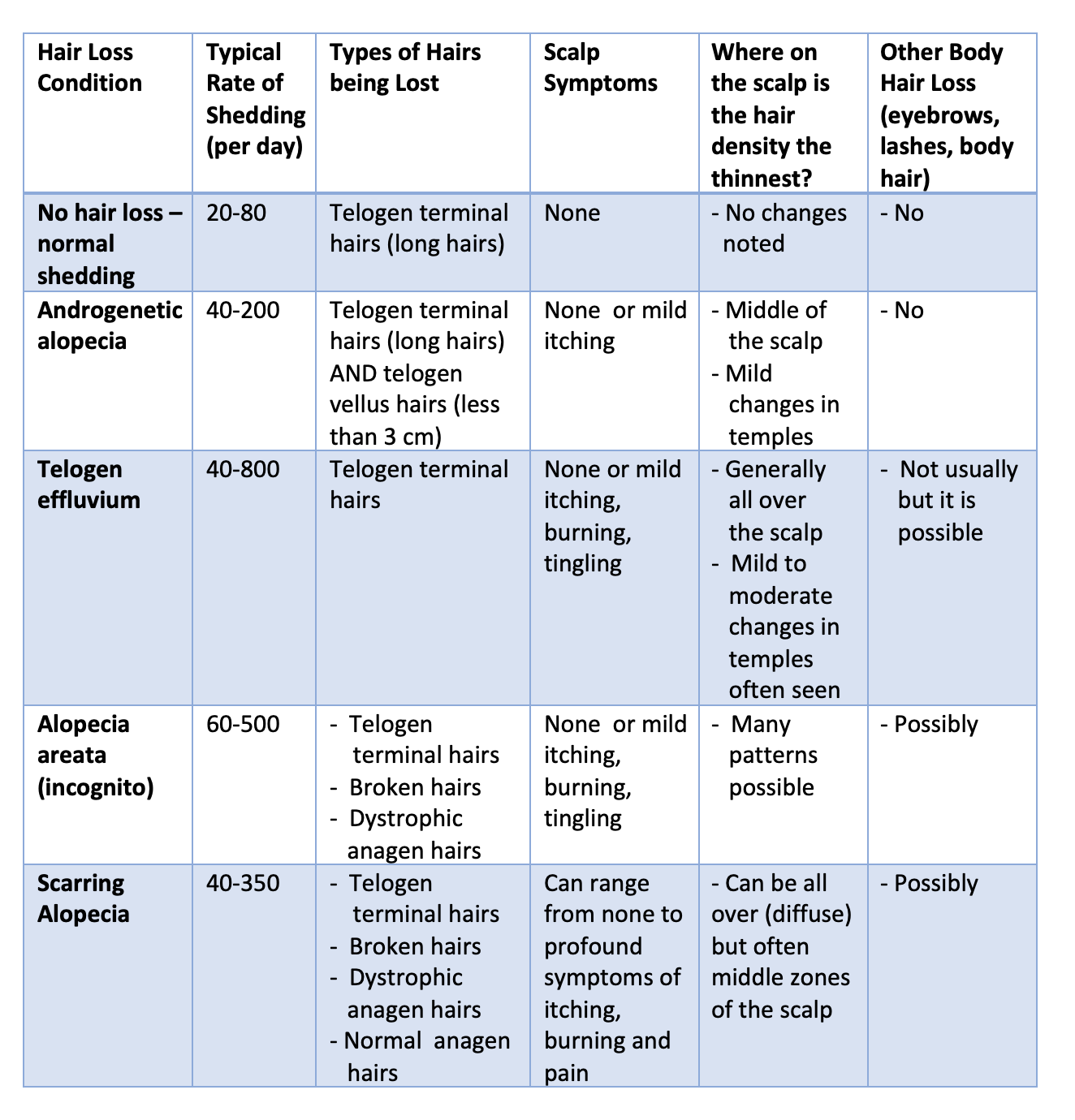
First - Normal shedding ranges from 20-80 hairs per day. Of course, if once shampoos every 2 days then that means the number is 40-160. If every 3 days then up to several hundreds hairs may be quite normal to be lost in the shampoo day. We lose more hair on the days we shampoo than on the days we don’t shampoo. It’s true that some lose up to 100 hairs per day but the reality is that if you average if out over a long time, it works out to under 100 hairs for most. This is the daily rate assuming one shampoos every day. If a person shampoos once per week, then they may lose 500 hairs easily that day without me even being concerned. shedding can vary across the menstrual cycle - especially after ovulation and in the days leading up to one’s period. This is normal. Other patterns are also possible.
Second - shedding can occur in other hair loss conditions and that rate of shedding can range from fairly normal to quite profound. Some individuals with telogen effluvium shed a little bit more than normal. However, some with TE shed massive amounts of hair. Generally speaking the rate of daily hair shedding in androgenetic alopecia is mild - but it must never ever be forgotten that AGA is one of the most common causes of slightly increased shedding in women with hair loss. Far too often we jump to the conclusion that a person with shedding has a diagnosis of telogen effluvium - nothing could be further from the reality. AGA must be on that list for women.
Third - the lengths of the hairs that are shed gives helpful information. If there are a few short hairs, one can’t conclude anything all that much. Everyone loses some short hairs and some long hairs - but mostly it’s long hairs that get shed. But if 20 %, 30 % or 40 % of the hairs that are being shed from the scalp are short less than 3 cm hairs, we need to at least start thinking about a diagnosis of androgenetic alopecia. A modified hair wash test can help quantitate this.
Fourth - the types of hairs that are being lost is helpful. We’ve talked about short hairs and long hairs in the section above. But long hairs can be telogen hairs, broken hairs and anagen hairs. If anagen hairs are being lost that look pretty normal anagen hairs, then scarring alopecia needs to be considered. If the anagen hairs are a bit “strange looking” then this may be a dystrophic anagen hair that one is seeing and a diagnosis of alopecia areata or scarring alopecia need to be reviewed. Finally, long hairs can be broken hairs. If broken hairs are what’s coming out of the scalp then alopecia areata, scarring alopecia needs to be considered - as does other entities like trichotillomania and chemotherapy induced loss and over use of heat or chemical styling practices. Of course, one usually knows if chemotherapy induced loss is a possibility because the patient will tell you if they have recently received chemotherapy treatment for cancer or not.
Fifth- the patient with shedding needs to figure out if they have hair loss all over or whether it’s occurring form one area more than others. If the patient feels that the back is much much less affected than the front of the scalp, the chances go up that the patient has androgenetic alopecia (AGA) as the cause of at least one of their diagnoses. Of course, they might still have TE and they might even have a scarring alopecia - but if there is a preferential reduction in density from one main area of the scalp that the person can point to with one finger - we need to consider the possibility of AGA.
Six - scalp symptoms can occur in any hair loss condition, but if they are profound and disabling and interfere with life then one needs to consider a scarring alopecia as the cause of shedding. Patients with AGA can have a little bit of itching. Patients with TE can have a little bit of itching. But massive 10 out of 10 itching, burning and pain is not a feature of AGA or TE. Conditions that give marked symptoms - that prompt people to put ice bags on their scalps - include scarring alopecias, allergic contact dermatitis, and scalp burns. Others exist too but you can see that AGA and TE are not part of this list.
Finally, the loss of other body hair can sometimes give clues. AGA is not associated with loss of eyebrows or eyelashes or body hair. Of course, if a patient says to me “oh, I do have eyebrow loss, come to think of it” this does not mean that they can’t have AGA. Eyebrow loss is common with age and so the simple finding of eyebrow loss does not mean that we have confirmed that the patient can’t have AGA . Not at all. It’s possible the patient has eyebrow loss as part of aging or over styling and now develops AGA too. But rapid loss of eyebrows, eyelashes and body hairs often points to an immune based reaction against hair follicles (with alopecia areata and frontal fibrosing alopecia being most common).
SUMMARY
I hope this helps. If you want to explore your shedding more, be sure to review with a hair specialist and pursue it methodically. You can look at the sizes of hairs being lost. You can measure the density on various areas of the scalp to determine if one area is thinner in density than another. You can review your symptoms. Together you can get a sense of whether your shedding is within the realm of normal or whether it is a reflection on an underlying scalp issue like AGA, TE or something else. If you feel that you have the same amount of hair on your head as age 27 and 17, then you are most likely dealing with the normal variations of shedding patterns. That’s really the most important question here.