Should I get another biopsy?
Should I get another biopsy?
I’ve selected this question below for this week’s question of the week. It allows us to review some concepts in interpreting biopsy results.
Question
I’m a 34 year old female with previously beautiful hair. My biopsy came back showing “non-scarring alopecia with features consistent with androgenetic alopecia.” I’m wondering if I should get another biopsy? Could it be wrong?
Answer
Thanks for the question.
Without knowing more about your medical history, and seeing your scalp (or photos), it’s difficult for me to say.
There are a number of possibilities here:
a) Your story and examination confirm you have androgenetic alopecia and doing a biopsy was not needed but simply served to confirm the diagnosis. Doing another biopsy would not be advised.
b) Your story and examination confirm you have androgenetic alopecia but there is a suggestion in the story or examination that a second diagnosis is also present. In this case, doing another biopsy could be a good idea if one is not 100% confident about this second diagnosis. If one is 100% confident in the second diagnosis, then another biopsy is not needed.
c) Your story and examination do not suggest androgenetic alopecia and there is a suggestion in the story or examination that a different diagnosis is present. In this case, doing another biopsy could be a good idea if one is not 100% confident about this diagnosis. If one is 100% confident in the diagnosis, then another biopsy is not needed.
I hope this helps. I don’t know your diagnosis because I haven’t seen your scalp and I don’t know your story. Certainly, if your practitioner is highly experienced in diagnosing women’s hair loss and says “This can’t be androgenetic alopecia” then I’m more likely to feel something is strange here and more likely to feel that a re-evlauation of things is needed. Early androgenetic alopecia is tricky to diagnose so many women have AGA even though it might not look like it.
If the practitioner is less experienced in diagnosing women’s hair loss, I’m less bothered by him or her saying “This can’t be AGA.” it’s tricky to diagnose some of the early forms of AGA. The reality is that if the terminal to vellus hair ratio on biopsy is dipping down below 4:1 and sebaceous glands are present in the biopsy there’s a good chance we’re dealing with AGA. The key question is whether this is the only diagnosis or the correct diagnosis.
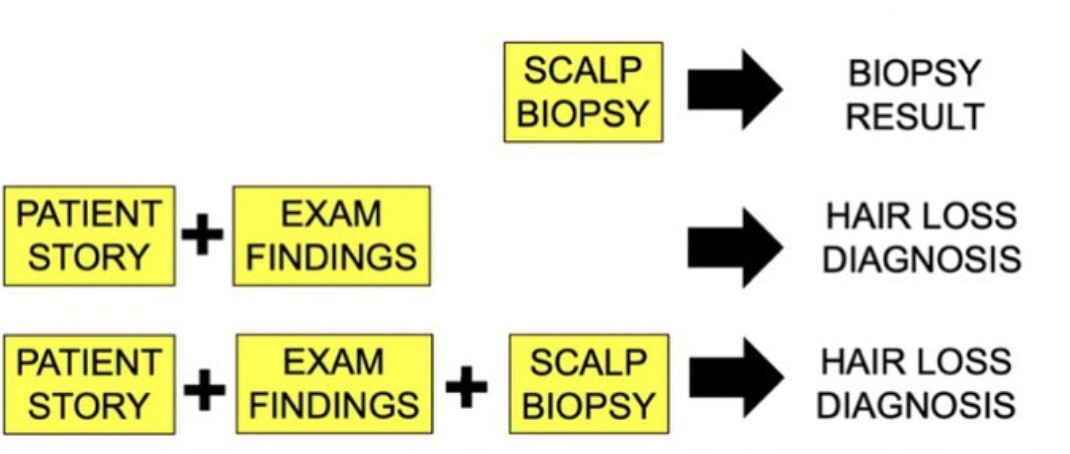
Finally, I’d like to point out that we don’t diagnose hair loss just with biopsy results alone. One needs to take the biopsy finding and see if it ties in with the history of hair loss and the clinical examination findings. I would never every commit to saying a person has a certain diagnosis without the chance to see their hair and know their story. Even with the biopsy sitting in front of me, I need to know the story and see the scalp.