Excessive Shedding in the 30's: Why is my hair still shedding?
Excessive hair shedding in the early 30s: What are the reasons?
I’ve selected this question below for this week’s question of the week. It allows us to discuss diagnosis of hair loss in women 30-40 years of age with chronic shedding. Here is the question….
QUESTION
Can oral vitamin + iron supplementation increase shedding the way minoxidil does?
I am a 35 years old female. I have always been under a lot of stress, especially in 2016-2017. In spring 2018 I noticed my hair got thinner (I always had rather fine hair); my scalp could be seen under direct light. I used castor oil and took spiruline tablets hoping it would improve; got the impression it did so I stopped. I was vegetarian then, too. I got preoccupied with the fear of getting bald, did a lot of research on the Internet that frightenend me even more and finally I got the courage to get an appointment with a dermatologist this summer (2020). She didn't notice hair loss (pull test); said my density was normal and scalp looked ok. She said it didn't look like AGA at all. She prescribed my iron supplementation (low ferritin (24)) and advised me to change my diet. I lack vitamin B12 too. From the end of July onwards I've been taking iron, spiruline, biotin and B12 supplementation. Since I didn't agree with the diagnosis ("no visible hair loss") I began counting the hair I'm shedding each day. The amount is horrible: it's more than 200 hair/day! The supplementation I'm taking and the changes I made to my diet don't seem to decrease the shedding at all. I've booked a appointment with anonther dermatologist for a second opinion (I'm truly terrified: my scalp feels strange; a bit of itching and burning + "crawling" sensations; my hair keeps falling out and for my dermatologist there's no problem...!) I'm surprised I still have hair left on my scalp when I see the amount that's falling every day...
I have read that those who use Minoxidil experience shedding in the first months which is a sign that new hair is on the way (I do see regrowth but it doesn't make my hair volume look any better). So I am wondering: can oral supplementation cause a similar shedding, which proves that the treatment is working? If not, what should I do? I got no "real" dagnosis; from what I read on the internet it seems to look like TE but how can I be sure?


I would like to add that from time to time I have small pimples on my scalp that come and go. Not a lot of them though, but they can be itchy. My skin (on face) is oily, I have the same sort of sores on my face from time to time too. I don't know if this information is important.
Thank you for reading and I hope you'll be able to answer my question since my own dermatologist doesn't seem to take my problem seriously...I think the thinning is all over, but mostly noticable on the top of my scalp and at the temples. My hair become very flat, no volume at all. I wash it daily because it greases very fast (eversince I was in my early teens).
ANSWER
Thanks for the question. There’s really two very good ways to determine the cause of your hair loss - and that is to share your story with a hair specialist and have him or her
1) Evaluate your scalp up close with “trichsocopy” (magnified imaging)
or
2) Perform a 4 mm scalp biopsy
So there is a way for you to get your answer.
I’d like to discuss several important things in the question you ask and the information you have submitted. Let’s get to it.
Before we do go further, I’d like to point out that the ideal way to diagnose hair loss is using what I termed the ”Diagnostic S.E.T.” I refer to these as the diagnostic “set” because theses 3 aspects all go together. These 3 items include:
1) the patient’s story
2) the findings uncovered during the process of the scalp examination including trichoscopy
3) the results of relevant blood tests.
The first letter of each of the three words 1) story, 2) examination and 3) tests spell out the word “S.E.T.” - again a helpful reminder of how the information obtained from reviewing each of these 3 aspects helps solidify a proper diagnosis.
AGA must be the Default Diagnosis in Women 30-40 with Increased Hair Shedding
I would need to examine your scalp to determine if you have androgenetic alopecia or telogen effluvium or both …. or some other diagnosis.
However, I strongly believe that the first diagnosis that must be ruled in or ruled out in any female patient with hair loss in the 30s is androgenetic alopecia. One must not move on until this issue has been fully settled. Once that it settled one can determine if the patient has or does not have telogen effluvium (with AGA or by itself ) and whether or not the patient has some other hair loss condition.
How does AGA present or ‘announce itself in women’? With shedding ! .. and with thinning in the top or often also diffusely!
How does telogen effluvium TE present itself or announce itself? With shedding ! …and with thinning diffusely !
It’s important to be aware that TE and AGA can look identical - at least at first glance.
What’s the most likely cause of hair loss in a 30-35 year old female with hair loss for 3 years and shedding and thinning? Androgenetic alopecia by far.
Of course, I can’t say what you have as I have not examined your scalp. But these are the principles that guide the entire discussion.
Therefore, the key question that must be asked in your story is “Does this patient have androgenetic alopecia (AGA)?” That’s the key question. That’s the number one question. The key question should not be what supplement can this patient take? ….. or what shampoo should this patient use? The key question is “does this patient have androgenetic alopecia?”
What is needed now is proof that you do have AGA or proof that you don’t have AGA. One should not rest until this question has been solved. Once we solve that question, we can move on to figuring out if any other diagnosis is present.
For now, we need to determine if AGA is present. That is what is needed now. Your doctors might be able to solve this with trichoscopy or they might need to solve it with a biopsy.
We can not always solve it with simply looking at the scalp from afar.
Only you know what your hair looked like before and your doctors do not. If you hair looks thinner to you but just fine to another person - then guess what? You still have hair loss.
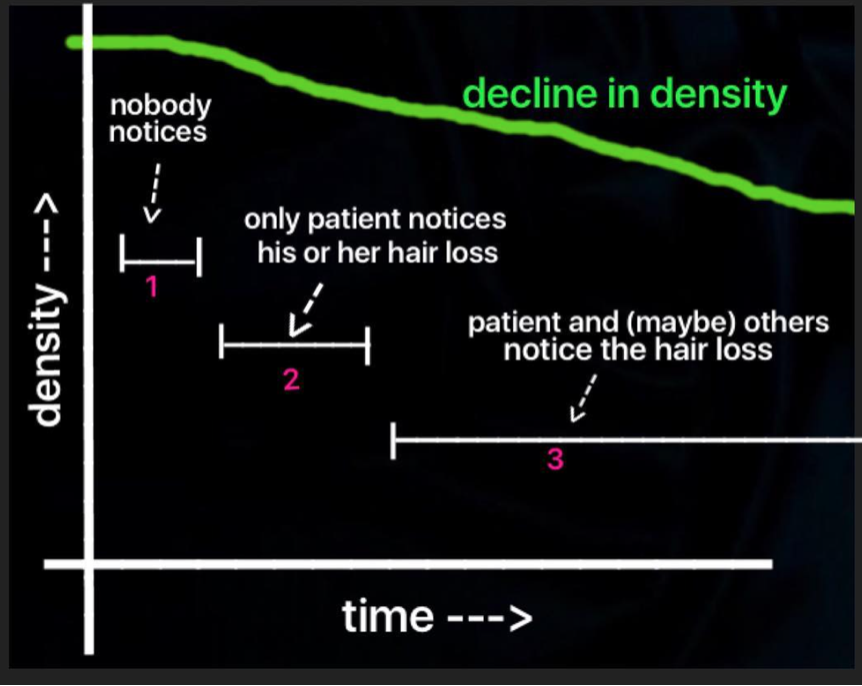
The Three Stages of Hair Loss
There are 3 stages of hair loss that I describe for patient’s with androgenetic alopecia. What is so important in your case is to determine once and for all as to whether you are in stage 2 AGA or whether you don’t even have AGA at all. Here are the stages.
Stage 1 of Androgenetic Alopecia
In stage 1, hair density is slowly reducing but the patient is unaware. There may be a slight increase in hair being shed in the shower or coming out daily in the brush. However, this generally goes by unnoticed by the patient. A biopsy can sometimes (but not always) capture a T:V ratio below 4:1 and some degree of miniaturization (and anisotrichosis) may be present. Much of the time it's challenging to confidently diagnose AGA in this stage. Some stay in stage 1 for a very long time; others just a matter of months.
Stage 2 of Androgenetic Alopecia
In stage 2, the patient first becomes aware that something is not quite right. They may see a bit more scalp showing when they look in the mirror. They may feel the hair does not feels as thick when they run their fingers through the hair. Under bright lights they may feel a bit more aware of these changes. When the hair is wet, the thinning is evident.
Nevertheless, in this second stage everyone else tells the patient they look fine. Some patients are told they are "crazy". Even some physicians will tell the patient they "look fine" and need not worry. Patients often feel isolated in this stage because nobody believes them when they say they are losing hair! A biopsy definitely shows a T:V ratio less than 4:1 and miniaturization is clearly seen in more than 20 % of hairs. Many never progress to stage 3 especially those with onset of AGA later in life.
Stage 3 of Androgenetic Alopecia
In stage 3, the hair loss has progressed to a stage where hair loss may become evident not only to the patient but also to others. Of course with use of various hairstyles, products, camouflaging agents it may still be possible to hide one's hair loss from others. As stage 3 progresses it becomes more and more difficult to hide hair loss.
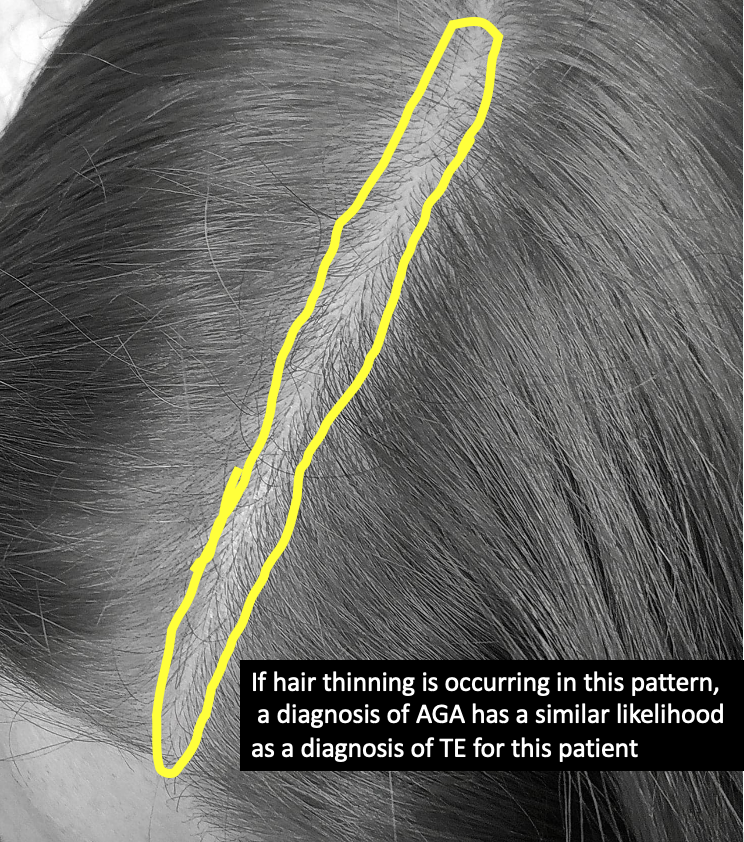
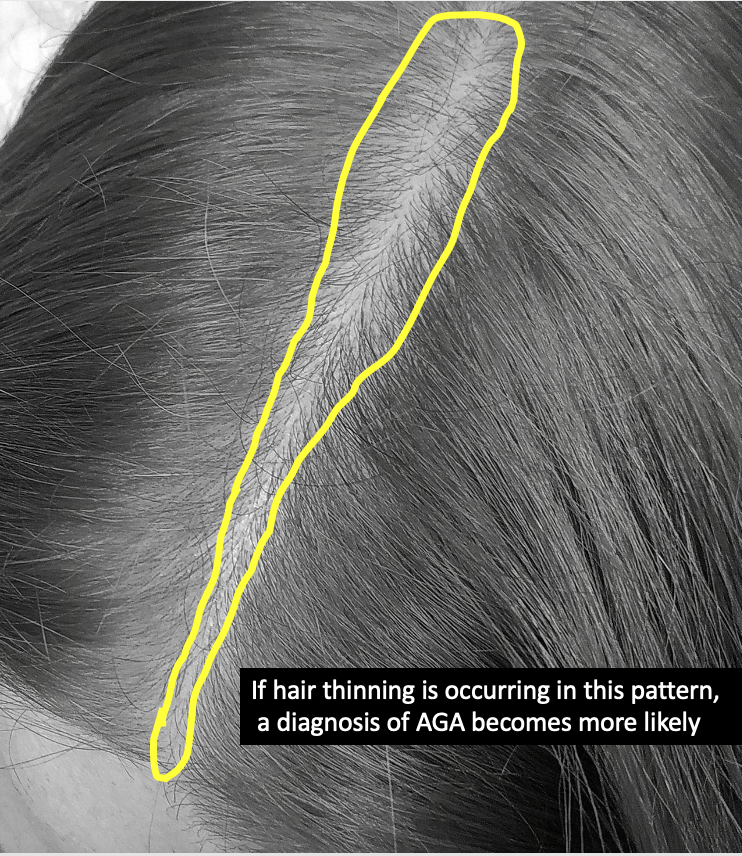
Understanding the Patterns of Hair Loss
Both AGA and TE can cause hair to look thinner. With AGA is typically affects the middle of the scalp whereas with TE is affects all of the scalp fairly equally. We call this a ‘diffuse’ pattern. AGA can sometimes have a diffuse pattern too but very often than not it affects the middle more than other areas. In addition, AGA often affects some areas of the middle a bit more than others.
Your photos show the hair parted in the middle. These types of photos are great for evaluating the scalp. If your part width at the back of the scalp seems smaller than the front of the scalp, the chances start to increase that you might have AGA. By part width, we simply mean the amount of scalp showing when you part your hair in the middle.
In your photos, it’s difficult to get a sense of the exact patterns because I only have photos of the middle. But when I look at these photos I do wonder whether the density towards the crown is a bit less than the density up front. In other words, it seems that even in the mid scalp the density is not reduced equally.
Summary: Putting it All Together
Thanks again for the question. Let’s review everything again.
1. You first asked if oral vitamins can increase shedding like minoxidil does. That answer is not usually. The mechanism is different.
2. You have high shedding rates so something is probably different with your hair cycles than it was 20 years ago.. One can shed 200 hairs daily in AGA and 200 hairs daily in TE so this information is not helpful to actually get to the diagnosis. You could have one, You could have both. You might have neither. Statistically speaking, a 30-35 year old female with shedding has either AGA or TE and with your history AGA is far more likely to be a diagnosis. Of course, we are not statistics and each person requires a proper examination.
3. You mention increased oiliness of the face so one needs to also consider whether you have a component of “seborrheic dermatitis”. This can increase these scalp sensations like you describe - and so can telogen effluvium. Your doctors can determine if you have SD by carefully examining your scalp.
4. Overall, it may be that you’ve had TE at some point in time - and perhaps you also have it now too. It may be that stress was a trigger before for a TE and perhaps maybe now you have different triggers that are causing a TE (such as lower iron). I suspect there was some component of TE back in 2016-2017 when your hair shedding stopped. Your doctors can evaluate these ‘triggers’ for shedding in greater detail. You may or may not need more blood tests but your doctors can review that in detail.
A full work up is needed at this point. You may need more blood tests. However, what you do need next is a thorough scalp examination with trichoscopy. If there is significant “anisotichosis” on trichoscopy then you may have AGA. I can’t tell these with your photos - it needs an up close examination. If it’s still difficult for your doctors to determine with trichsosopy, then a scalp biopsy (with use of horizontal sections) is going to be helpful. The pathologist can determine the number of large terminal hairs and tiny vellus hairs and the number of telogen hairs. A terminal to vellus hair ratio of less than 4:1 usually signals a diagnosis of AGA in women. You can review more about scalp biopsies here Scalp Biopsy Interpretation
I hope this helps and thank you again for the question.