Low Dose Oral Minoxidil: Is 1 mg better than 0.25 mg for Women with Female Pattern Hair Loss
Low dose oral minoxidil is increasingly used in treating female pattern hair loss. We have reviewed the topic in the past several times given just how important it is for clinicians to understand the use of oral minoxidil. (see prior articles “Top 10 Things You Need to Know About Oral Minoxidil For Hair Loss” and “5 Common Mistakes in Prescribing Oral Minoxidil for Women’s Hair Loss” Despite the interest in oral minoxidil optimal dosing is still not clear. Prior studies suggested that 1 mg was similar to 5 % minoxidil for women.
Silva et al, 2022
Authors from Brazil performed a 24-week randomized double-blind clinical trial to evaluate the efficacy and safety of 1 mg and 0.25 oral minoxidil for the treatment of FPHL. Thirty women with FPHL were randomly assigned to receive 1 capsule of compounded LDOM 0.25 mg or 1 mg once daily for 24 weeks. In order to evaluate improvement authors examined a variety of measures including hair counts, photographs, hair shedding scores and quality of life changes.
Study Results
26 patients actually completed the trial and four dropped out. Female patients using 1 mg and women using 0.25 mg were similar in baseline characteristics indicating fair comparison. Female patients using 0.25 mg did not have an increase in hair counts while female patients using the 1 mg dosing of oral minoxidil did show an improvement in hair counts.

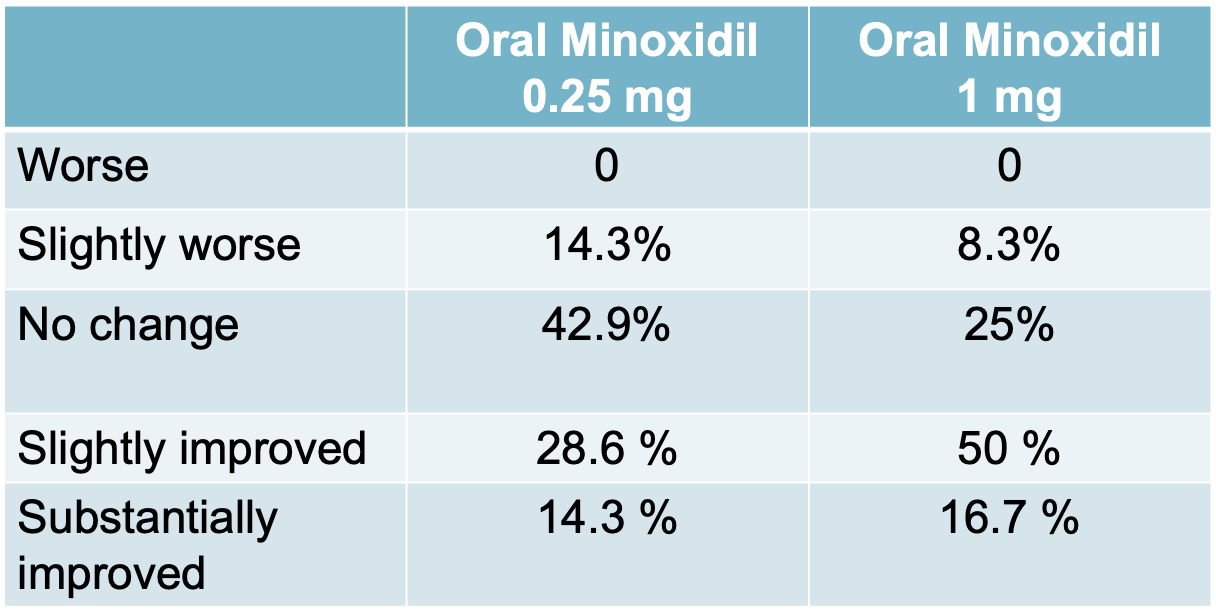
In terms of improvement, global photographic improvement was documented by 3 board certified dermatologists blinded to the treatment groups. 42.9 % of participants using 0.25 mg had an improvement (either slight or substantial) compared 66.7 % of those using 1 mg.
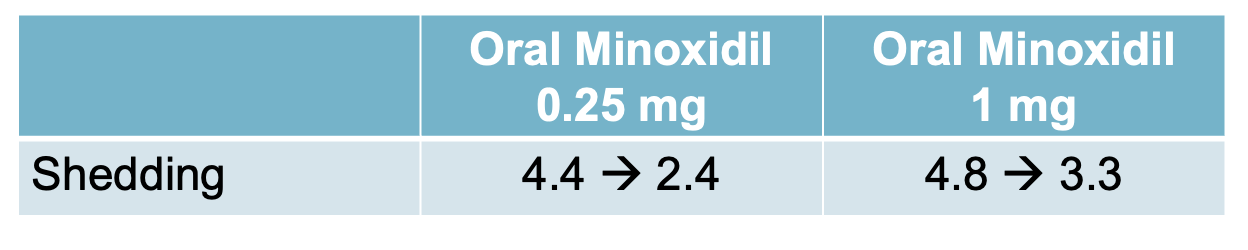
Both treatment groups had decreased shedding and improvement in quality of life scores. Below the shedding scores using the Sinclair shedding scale are shown:
Conclusion
This is an interesting study which points to potentially better improvement in hair density when treating female androgenetic alopecia with 1 mg compared to 0.25 mg. There are several important limitations to this study that should be noted. Overall the study is small so it’s not clear if other differences would be seen with larger number of participants. In addition, there is no placebo control, so it’s not clear what proportion of benefits are really attributed to the drug.
Nevertheless, the study affirms that low dose oral minoxidil 0.25 and 1 mg probably both do something positive, although 1 mg is likely superior. One should not negative the potential benefits of 0.25 mg oral minoxidil - four times more medicine does not equate to four times better responses.
REFERENCE
Silva et al. Randomized clinical trial of low-dose oral minoxidil for the treatment of female 3 pattern hair Loss: 0.25 mg versus 1 mg . Journal of the American Academy of Dermatology; Online Jan 2022.
This article was written by Dr. Jeff Donovan, a Canadian and US board certified dermatologist specializing exclusively in hair loss.