What is the reason for my hair loss?
Why am I shedding ?
I’ve selected this question below for this week’s question of the week. It allows us to discuss shedding issues in women with hair loss.
QUESTION
Hi!
I am a 42 year old women and have been shedding about 200 hairs a day since March, 2020. I have seen 4 dermatologists and my General Practitioner and they have different diagnoses from TE to FPHL or a combination of both. Prior to March, 2020 I was under extreme stress which started in November 2019. In March 2020 my hair loss was sudden and I have had diffuse shedding since then for the past 10 months. I have always had full, thick and healthy hair and no issues with my hair until the past 10 months. There is no family history of hair loss and my bloodwork came out normal.

Increased hair shedding.
I have been taking vitamins, biotin and Lysine (since June 2020) daily. I am washing my hair every other day, air dry my hair and do not use styling or heating products and eat healthy. I am also taking spirolactone since December 2020 (one month as of today). My dermatologist suggested I take spirolactone (50 mg twice a day) because I have irregular periods. My hair loss slowed down in September 2020 to about 100 hairs a day and went back up to 200 plus in November 2020. I am experiencing itchiness, pins and needles sensation on my scalp and my hair texture changed from straight to wavy for the past 10 months. My hair is also now flat, dull and I have some dandruff that comes and goes. My middle part is widening (compared to pre-March 2020 before the shedding) and with the ongoing shed the part has somewhat looked the same since March.


I lost about 30% of my hair and cannot style it the way I used to because of the thinning in the front. The last two dermatologists I saw performed a pull test and scalp examination and one of them said it is CTE and that there is nothing I can do but wait it out. The other doctor said it's FPHL and that she can tell just by looking at the front of my hair because of the way its thinning. I do see hair growth and my hair is full of static with short hairs coming out but I am also losing a lot of hair in all different lengths including short ones every day. I am frustrated because it has been 10 months and my shedding is not stopping. I do not know which diagnosis is right and what treatment I should start. Also It would be great for the itching and "pins and needle" feeling on my scalp to go away...
Thank you for reading and I'm so happy to find this website.
ANSWER
Thanks for the question.
I’d like to discuss several important things in the question you ask and the information you have submitted.
Before we do go further, I’d like to point out that the ideal way to diagnose hair loss is using what I termed the ”Diagnostic S.E.T.” I refer to these as the diagnostic “set” because theses 3 aspects all go together. These 3 items include:
1) the patient’s story
2) the findings uncovered during the process of the scalp examination including trichoscopy
3) the results of relevant blood tests.
The first letter of each of the three words 1) story, 2) examination and 3) tests spell out the word “S.E.T.” - again a helpful reminder of how the information obtained from reviewing each of these 3 aspects helps solidify a proper diagnosis.
There is lots more to your story that I need. I would want to know exactly what your lab tests showed and which ones were tested. In about 20 % of patients who tell me they had blood tests and all came out normal, the labs are either insufficient (more are needed based on their story and examination) or the labs are not in fact really normal. I always like to see the labs. I would want to know about other symptoms like joint pains, headaches, fatigue, weight loss, eyebrow changes, eyelashes changes, body hair changes, nail changes, and rashes.
I strongly suspect that androgenetic alopecia with seborrheic dermatitis are part of the diagnoses. The 2 key questions here in your case are:
Do you have really have telogen effluvium as well ?
What really is the reason for the ‘pins and needles’ sensation ?
Let’s look at a few key points.
POINT 1. Androgenetic alopecia (female pattern hair loss) appears to be at least one of the diagnoses.
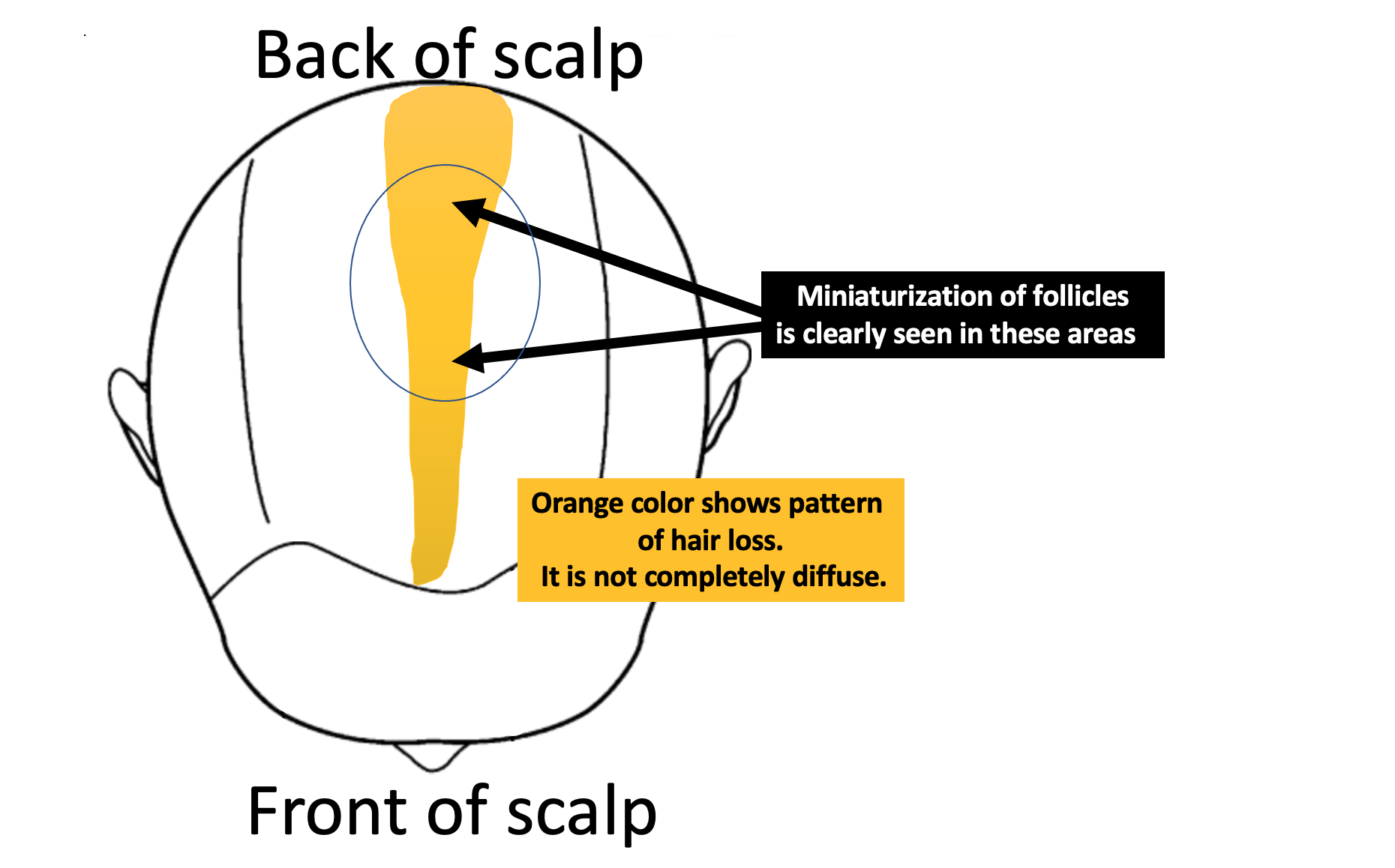
I do think that at least one of the diagnoses here is androgenetic alopecia (also called female pattern hair loss, FPHL). The widening of the part does not itself mean the diagnosis is AGA. however, the pattern of the part widening is not the same front to back. There is a slight increase in thinning noted in the mid scalp and crown compared to the frontal one third of the scalp. This leads me to believe there is a patterned nature of the hair loss. I’m open to the possibility that some of the hair loss is diffuse in nature (ie all over) but some is likely not. In other words, I don’t think this is entirely a diffuse type of hair loss.
Also, when I look up close at the images, it’s clear that some follicles are thinner than others. This is a phenomenon called anisotrichosis and is a feature of AGA. Some hair follicles are miniaturization (getting thinner).
Women with AGA often experience shedding of hair in the early stages and shedding can fluctuate in intensity. Other hair loss conditions can cause shedding as well so we’ll address that in just a moment. Women with AGA often notice that the texture of hair changes. There are many such patterns of texture change and a change from straighter to curlier is quite common as you too have described.
The fact that you note increasing numbers of short hairs is not confirmatory for a diagnosis of AGA but certainly is supportive of this diagnosis.
POINT 2: Seborrheic dermatitis/dandruff is likely another diagnosis.
I agree with you that dandruff (or its close cousin called seborrheic dermatitis) is likely present. Flakes are noted in some of the photos. I’d need to perform trichoscopy to confirm this diagnosis but it appears to be a component of the issues present. Mild dandruff is not usually a cause of hair loss but it certainly can cause all sorts of scalp symptoms. To eliminate the possibility that dandruff or seborrheic dermatitis is contributing to symptoms, I often encourage my own patients to aggressively treat their seborrheic dermatitis so we can remove this as a factor. Shampoos with zinc pyrithione, ketoconazole, selenium sulphide or ciclopirox can be used 2 times per week and left on 90 to 120 seconds before being rinsed off. The duration that these shampoos are left on the scalp can certainly be increased but I don’t recommend that to start with as many antidandruff shampoos can be drying and then the dryness starts causing itching and symptoms. I often recommend to my own patients that 5-10 drops of betamethasone valerate lotion 0.1 % can be applied in the scalp after their hair is shampooed and dried. This is a weak steroid and can be safely used for 2 week periods to help settle itching. If the use of shampoos settles the itching, tingling and pins and needles, then it’s not needed.
POINT 3: Telogen effluvium could be present.
Telogen effluvium is one of those conditions that can come and go. Sometimes it’s easy to prove a TE is present and sometimes it’s a bit more challenging. It could be that a TE was present when your AGA first started. You were under extreme stress in November 2019 and yes this could most definitively give shedding in March 2020. Telogen effluvium usually follows 2-3 month after some kind of trigger and can last 3-6 months or more. Other causes of telogen effluvium are low ferritin levels, thyroid issues, medications, diets, weight loss and internal illness. I don’t really have enough information to evaluate these other issues so I’ll go with your assessment that your blood tests were normal. Hopefully you had a reasonable set of tests including TSH, ferritin, CBC. With your irregular periods you describe it would make sense to have FSH, DHEAS, testosterone. One needs to consider whether you are entering a perimenopausal transition and how this could contribute to hair shedding and AGA. With any pins and needles sensation, it’s nice to know that liver enzymes (AST, ALT) are normal and that kidney function is normal (creatinine).
Telogen effluvium can sometimes precipitate or accelerate an underlying AGA. This is a well accepted phenomenon. it does not happen to all women with AGA. However, women with shedding who have AGA that is about to begin (ie very early onset AGA) often find that the AGA component of the hair loss gets sent into a more rapid speed of development if a TE is present. This could be a feature here.
With your normal blood tests, it’s unlikely that a TE is still driving hair loss all this time. Not impossible of course, but unlikely. What is more likely is that AGA is not fully being treated. Spironolactone helps but does not fully suppress AGA in all women at 50 mg twice daily. Sometimes higher doses are needed OR other treatments for AGA are needed (other anti androgens, laser, minoxidil, etc)
POINT 4: If you want to assess the degree to which AGA and TE are present, you could have a biopsy or 5 day modified hair wash test (or a proper trichoscopic examination). I don’t think these are really needed.
For your physicians/specialists who think that AGA is not a diagnosis here for you, a biopsy or 5 day modified hair wash test could help prove them wrong (… or prove them right!). This is a wonderful test but adds to the stress of collecting hairs so I’m not always in favour of it. Biopsies leave scars but if interpretted by a knowledgable dermatapathologist, they can be very helpful.
But, let’s be clear. A biopsy showing a terminal to vellus hair ratio of less than 4:1 taken from your mid scalp area puts to rest any argument about whether AGA its present of not. End of discussion. A 5 day modified hair wash test (done properly !) showing less than 100 hairs and more than 10% hairs being tiny 3 cm hairs also points to an underlying AGA.
Of course, simply examining the scalp with trichoscopy can also confirm this diagnosis but not all specialists are skilled with trichoscopy. If a specialist knows how to use a handheld dermatoscope, we don’t even need biopsies or hair collections to diagnose AGA. If they don’t then yes, we need to go to the extra effort to prove it.
POINT 5: The ‘pins and needles’ is a bit trickier given how many conditions can cause this.
There are a very large number of conditions that can cause pins and needles in the scalp. Stress can cause it. AGA can cause it. TE can cause it. Alopecia areata can cause it. Dandruff can cause it. Scarring alopecias cn cause it. The list is long and includes issues even outside the scalp like cervical spine disease.
I would need to know more about your story and carefully examine the scalp and eyebrows and eyelashes and nails to get a sense of what is causing this.
For pins and needles sensations, I usually advise treating any dandruff or seborrheic dermatitis and using a few drop of betamethasone lotion as outlined above. If it’s still there and the patient has AGA, I usually recommend treating the AGA more aggressively. This often help stop pins and needles. Low level laser, minoxidil and other antiandrogens can be considered.
Conclusion/Summary
Thanks for the question. I hope this helps you in your search for answers and helps with further discussion with your doctors. I think it’s really important for you and your doctors to feel confident with the diagnosis and not proceed with any sort of “maybe.” It would appear that AGA is a component of the issues here but if there is any doubt, a trichoscopic examination, biopsy or 5 day modified hair wash test can help confirm this.
Photos are really important moving forward to document changes - hopefully for the better.
if spironolactone is not fully helping then you and your dermatologists might discuss together whether or not to increase the dose or whether other treatments need to be considered. These include topical minoxidil, oral minoxidil other topical or oral antiandrogens and low level laser. PRP can be considered too. The important thing to note about minoxidil, laser and PRP is that if there is any amount of chronic shedding issue present these treatments can help promote more normal shedding patterns. This is assuming all your blood tests are normal. If any of your blood tests are abnormal and if, in fact, you have not had a proper work up then those issues need to be addressed first. it sounds like you’ve had a good set of blood tests through all the doctors you have seen.
Thank you.